Maxillofacial phlegmon: causes and dangers
The vast majority of phlegmons (more than 90%) are odontogenic in nature, that is, they arise due to a tooth that is not treated in time, destroyed by caries or periodontitis. The causative agents of inflammation - staphylococci, streptococci, anaerobic and putrefactive microorganisms - penetrate from the affected tooth root into the tissues of the perimaxillary region due to the peculiarities of the outflow of lymph and venous blood. Another difference between phlegmon and an abscess is that it develops against the background of a significant decrease in immunity, while an abscess can form in a patient with normal protective reactions of the body.
Cellulitis of the maxillofacial area is a dangerous condition that requires serious surgical intervention. The severity of the patient’s condition is determined by the degree of neglect of the process and general intoxication of the body. In addition, nerve endings are concentrated in the jaw area, so a diffuse purulent inflammatory process brings unbearable pain and physical suffering to a person. Vital functions are impaired - swallowing, chewing, speaking, breathing. And a large number of venous plexuses favors the rapid spread of the process and its transition to vital organs and systems. The most severe complications of this disease:
- phlebitis;
- thrombophlebitis;
- mediastinitis,
- abscesses of internal organs;
- meningitis;
- meningoencephalitis;
- sepsis.
Cellulitis is especially severe in children or if it is caused by anaerobic microorganisms.
Localization and forecast
The localization of each of the phlegmons, which can be primary or secondary , is determined by the anatomical and topographic boundaries of the cellular spaces, which are determined by the muscles, intermuscular fascia, bone structures, and neurovascular sheaths.
Paramaxillary phlegmon (abscesses) include, in addition to those considered, phlegmon (abscess) of the buccal region, phlegmon (abscess) under the temporal region, pterygopalatine fossa, temporal region, abscess of the hard palate.
A peculiarity of the buccal area is the presence of a fatty lump of Bisha enclosed in a thin fascial sheath, which with its processes penetrates into neighboring spaces and causes the spread of the infectious process in them. In addition, the presence of facial veins in this area threatens their phlebitis and the possible spread of infection to the sinuses of the brain. The reasons for the development of purulent processes in this area are the teeth of the upper jaw affected by periodontitis, less often the lower third molar, periostitis and osteomyelitis of the upper jaw. Non-odontogenic causes of the process include the presence of acute purulent sinusitis and injection infection.
The buccal region does not have powerful and significant muscle masses, the tissue is loose, without pronounced interlobular fascial plates. The facial and buccal muscles do not pose serious obstacles to the spread of the inflammatory process. Therefore, the clinical signs of phlegmon (abscess) of the buccal area are quite characteristic and are manifested by severe hyperemia, covered with shiny skin, the infiltration of which leads to swelling and closure of the eyelids, deformation of the lip and wing of the nose. Fluctuation can be detected already in the early stages of the disease. When the abscess is localized closer to the mucous membrane of the cheek, skin hyperemia is less pronounced, but there is a bulging of the mucous membrane and its intense hyperemia along the upper and sometimes lower fornix of the vestibule of the mouth with early signs of fluctuation.
The surgical approach is determined by the predominant localization of the lesion, but preference, taking into account cosmetic requirements and the risk of damage to the branches of the facial nerve, is given to the intraoral one. An incision is made along the upper vestibule of the oral cavity or along the mucous membrane of the cheek in the place of greatest bulging, taking into account the direction of the duct of the parotid gland, then the purulent focus is bluntly opened, emptied and drained. In case of insufficient drainage, an incision is used along the lower orbital edge, nasolabial fold. In rare cases of a common process, a combination of intraoral and external approaches is used.
The prognosis for the treatment of phlegmon (abscesses) of the buccal area is usually favorable. More dangerous in nature and difficult to diagnose are phlegmon (abscess) of the infratemporal space and pterygopalatine fossa, often secondary in origin, but they can be caused by a process developing from the upper molars, or a violation of the technique of tuberal anesthesia. Their danger lies in the fact that the spaces have direct communication with the orbit (inferior orbital fissure) and the cranial cavity (foramen rotundum). Difficulties in diagnosis are due to the paucity of clinical manifestations due to the deep localization of the abscess and a powerful group of masticatory muscles (temporalis, pterygoid). The predominant symptoms are significant pain in the depths of the face and severe inflammatory contracture of the masticatory muscles. Hyperemia and skin tension are almost not observed. When the cheek is moved outward along the upper fornix of the vestibule, one can see hyperemia and bulging of the mucous membrane behind the tubercle of the upper jaw, between it and the edge of the branch of the lower jaw, where sharp pain is detected on palpation. With more pronounced inflammatory changes, an hourglass-shaped swelling appears in the temporal and infratemporal regions, and swelling of the infratemporal region. The pain intensifies and radiates to the eye and ear. There is some discrepancy between pronounced disturbances in the general condition and minor local symptoms.
Opening phlegmon of these localizations is possible using several approaches:
1. an incision along the upper arch of the vestibule of the oral cavity behind the tubercle of the upper jaw with blunt penetration behind it backwards, inwards and upwards;
2. external access with resection of the zygomatic arch and coronoid process from an incision parallel to the zygomatic arch;
3. an incision from the submandibular approach with cutting off the pterygoid muscle.
The prognosis for delayed diagnosis and insufficient drainage is serious, including the development of life-threatening conditions due to the possible spread of the process into the tissue of the orbit, cavity and sinuses of the brain.
Secondary phlegmon can also develop in the temporal region, where the cellular spaces are located in several layers: between the muscle and the skin, between the fascial sheaths of individual muscle groups, between the muscle aponeurosis and the scales of the temporal bone. Finally, the process can involve all layers of fiber. The degree of clinical manifestations is determined by the affected area. The more superficial the process, the more pronounced its manifestations: hyperemia, skin infiltration, spreading edema, contracture and pain are less pronounced. With deep and total involvement of fiber in the process, hyperemia is not expressed, but the pain intensifies, muscle contracture increases to the point of complete impossibility of jaw movements, an “hourglass” symptom, hyperemia, and bulging of the mucous membrane of the upper vestibule behind the tubercle of the upper jaw may be observed. To ensure sufficient conditions for outflow, incisions are used parallel to the zygomatic arch above it, fan-shaped incisions in the temporal region with dissection of the aponeurosis of the muscle and separation of its bundles, an arcuate incision along the upper border of the attachment of the muscle of the temporal bone with dissection of the aponeurosis to the bone. This incision must be combined with a contraperture - an incision above the zygomatic arch. The prognosis for the above reasons is also serious.
Less dangerous and easier to diagnose is an abscess (phlegmon) of the zygomatic region . The superficial location of the process causes quite characteristic manifestations. Drainage is carried out from incisions in the place of greatest tissue protrusion, taking into account the location of the branches of the facial nerve. It is possible to drain from the incision along the nasolabial fold, which is cosmetically more justified, or along the transitional fold of the upper arch of the vestibule. The prognosis is usually favorable. Thus, phlegmons (abscesses) of the perimaxillary localization are varied in their course and possible complications. Diagnosing them is sometimes difficult. Therefore, the examination of the patient must be carried out carefully and comprehensively, which will avoid errors in treatment.
An abscess of the hard palate most often develops from the palatal roots of molars or infection during palatal anesthesia. It is easy to diagnose as it forms between the bony base of the palate and the immobile mucous membrane. Opening the abscess to ensure outflow should not be done with a linear incision, but with excision of a crescent-shaped triangular flap of the mucous membrane at the site of the greatest bulge. Otherwise, the edges of the wound stick together and outflow becomes impossible.
Our team of doctors
Maxillofacial surgeon, Implantologist
Bocharov Maxim Viktorovich
Experience: 11 years
Orthopedist, Neuromuscular dentist
Stepanov Andrey Vasilievich
Experience: 22 years
Orthopedic dentist
Tsoi Sergey Konstantinovich
Experience: 19 years
Endodontist, Therapist
Skalet Yana Alexandrovna
Experience: 22 years
Endodontist, Therapist, Orthopedist
Varvyanskaya Anastasia Andreevna
Experience: 6 years
Dentist-orthodontist
Enikeeva Anna Stanislavovna
Experience: 3 years
Diagnostics
In a clinical blood test with phlegmon, changes characteristic of purulent inflammation are present: leukocytosis, neutrophilia and a sharply increased ESR. When examining blood serum, C-reactive protein is detected.
The diagnosis is made by a dentist-therapist. It is based on the clinical manifestations of the disease, the patient’s subjective complaints, as well as the results of the necessary laboratory tests, which allow us to draw conclusions about the extent of the disease, the severity of the inflammatory process, and evaluate the effectiveness of therapy.
It is important not to confuse phlegmons and abscesses with facial boils and carbuncles, erysipelas, as well as inflammation of the submandibular and parotid salivary glands, since their external manifestations at the initial stage of the disease may be similar.
Symptoms
Phlegmon of the perimaxillary region, unlike an abscess, develops rapidly and is characterized by severe intoxication. Its main clinical manifestations:
- infiltration on the affected area of the face or neck;
- hyperemia, swelling, soreness of the skin at the site of inflammation;
- high body temperature;
- rapid pulse;
- severe pain when chewing, swallowing, talking;
- spasm of the muscles responsible for opening and closing the mouth (trismus);
- increased salivation;
- weakness;
- chills;
- pale skin;
- loss of appetite;
- sleep disorders;
- enlargement of regional lymph nodes;
- facial asymmetry.
Periandibular phlegmon, photos of which can frighten impressionable people, is always accompanied by an increased number of leukocytes and neutrophils in the blood, a shift in the leukocyte formula to the left and an increased ESR value. The diagnostic sign of phlegmon in the blood serum is C-reactive protein. Protein and white blood cells also appear in the urine.
Classification of phlegmon
Several approaches are used to classify phlegmon. So, depending on where the infection entered the body, pathology is divided into 3 groups. Primary (infection occurred from the outside), secondary (if the infection migrated from another part of the body) and chronic (when a new phlegmon appeared due to the fact that the old one was not completely cured).
Depending on the location, pathology is divided into:
- Subcutaneous.
- Subfascial.
- Memuscular.
- Perinephric.
- Retroperitoneal.
- Affecting the feet, hands, etc.
According to the degree of development, phlegmon is distinguished:
- Serous. The initial stage, the only external manifestation of which is a slight swelling. While leukocytes and watery fluid actively accumulate inside.
- Purulent. The skin over the affected area begins to turn red, because... in addition to the liquid, pus gradually accumulates underneath it. The main symptoms are pain when touching the growth and fever.
- Putrid. Due to constant contact with pus, tissues begin to break down, releasing gas with a pungent, unpleasant odor. Intoxication of the body occurs.
- Necrotic. The affected tissues gradually die. Often forming abscesses.
Treatment
Despite the severity of the disease, in general, with timely treatment, perimandibular phlegmon has a favorable prognosis. Treatment is carried out only in a hospital setting, but at the initial stage everything is often limited to the use of conservative methods - antibiotic therapy, the prescription of restoratives, vitamins, and a special diet. But if the process has already started and the spread of infection is observed, complex surgical treatment is indicated, which includes the following points:
- opening the inflammation site under general anesthesia;
- cleansing the wound from pus;
- installation of drains for drainage of wound contents;
- daily treatment with bactericidal solutions;
- powerful antibiotic therapy - often a complex of several drugs is prescribed;
- detoxification of the body;
- use of antipyretic and painkillers;
- prescription of immunomodulating, restorative agents, vitamins;
- physiotherapy – ultraviolet irradiation, UHF, magnetic therapy, etc.
If treatment is successful and there are no complications, the patient’s recovery occurs on average in 14-21 days.
Phlegmons of the pterygopalatine and infratemporal fossae
The local symptoms of phlegmon of the pterygoid - palatine and infratemporal fossae are essentially the same, because these 2 anatomical and topographic spaces are widely interconnected.
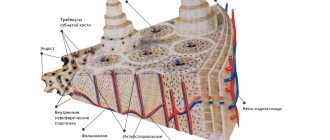
Scheme of localization of phlegmon in the pterygopalatine and infratemporal fossae:
1. head of the mandible
2. inflammatory infiltrate
3. medial pterygoid muscle
Inflammatory infiltrates formed in the infratemporal and pterygopalatine fossae are located between the posterior wall of the maxillary bone and the lateral pterygoid muscle, the lateral plate of the pterygoid process of the sphenoid bone, then spreading along the branch of the lower jaw along the course of the pterygoid muscle. The spread of the inflammatory infiltrate into the pharyngeal fossa, the peripharyngeal space and the infratemporal fossa usually does not occur from here, since the powerful aponeurotic and fascial formations passing here exclude such a possibility.
Phlegmon of the infratemporal and pterygopalatine fossae can be the result of infection of the fiber from the periapical tissues, more often 8I8, less often - 7 6I6 7 teeth. The inflammatory process can spread from other adjacent anatomical and topographic spaces, in particular from the pterygomaxillary, where the most common cause of the development of phlegmon of the infratemporal and pterygopalatine fossae is infection of the hematomas formed here during the vicious implementation of anesthesia of the tissues of the upper jaw. By penetrating deeply into the infratemporal fossa with an injection needle, the doctor easily injures the venous plexus, and the developing hematoma becomes infected. Cellulitis of “injection” origin is formed. Therefore, the sign of a “causal” tooth in the etiology of phlegmon of this localization is relative. The sign of inflammatory infiltrate when examining the patient’s face is weakly expressed or not determined. However, palpation of tissue along the transitional fold of the vestibule of the mouth in the area of the lateral teeth of the upper jaw always reveals infiltration and pain. The infiltrate can spread, descending along the anterior edge of the mandibular ramus. The sign of inflammatory contracture of the lower jaw is expressed due to the involvement of primarily the lateral pterygoid muscle in the process; an attempt at lateral movements to the “healthy side” is unsuccessful. The opening of the mouth may also be limited to some extent.
Thus, with phlegmon of the pterygopalatine and infratemporal fossae, the sign of the “causal” tooth is relative; the sign of inflammatory contracture of the lower jaw is positive due to the involvement of the lateral pterygoid muscle in the inflammatory process, but mouth opening can be maintained in full; the sign of inflammatory infiltrate is negative. There is no sign of difficulty swallowing.
Operative access – intraoral. An incision of the mucous membrane 2-3 cm long is made along the transitional fold in the posterior part of the vault of the vestibule of the mouth. Then, advancing the rasp to the bone, they go deeper into the tubercle of the upper jaw, thus penetrating into the infratemporal and pterygopalatine fossae. After evacuation of the pus, the wound is drained. The prognosis is usually favorable, but one must keep in mind the possibility of rapid spread of purulent exudate to the temporal region, orbit and pterygo-maxillary space.
What types of diseases exist
Phlegmon is classified according to several criteria.
By localization
- superficial: local symptoms predominate - pain, swelling, fever up to 39˚C, chills,
- deep: general symptoms are more pronounced - the temperature rises sharply to 42˚C, the heart rhythm is disturbed, blood pressure drops, and difficulties with breathing and urination occur.
By stages of development
- acute: the temperature rises sharply, swelling and hyperemia of the soft tissues are pronounced,
- chronic: the infectious focus is compacted, it is characterized by cyanosis, pain when pressing,
By type of exudate (accumulated liquid)
- serous,
- purulent,
- necrotic.
The main reasons for the development of pathology
The main cause of phlegmon is the penetration of microbes into certain tissues of the body. This can occur in the presence of untreated dental diseases - odontogenic type, or through lymph and blood flow due to injuries to the mucous membrane - non-odontogenic type. The disease is provoked by the following factors:
- poor or complete lack of oral care, especially after tooth extraction and other situations associated with surgery. That is, most often phlegmon is a complication of the underlying disease, including its treatment,
- advanced diseases of the teeth, gums and oral cavity: caries, pulpitis, periodontitis, gingivitis, periodontitis, stomatitis,
- problematic eruption of wisdom teeth,
- injury to soft tissues after tooth extraction: for example, on the first day the patient began to actively rinse the wound and washed out the protective clot, or chewed on the side of the jaw where the operation had recently been performed,
- ignoring the dentist’s recommendations by the patient after tooth extraction or other intervention,
- failure to comply with aseptic standards when performing dental procedures by a doctor,
- the presence of boils, pustules, ulcers on the oral mucosa or skin,
- injuries to the oral mucosa: for example, with regard to complex tooth extraction, the doctor could carry out the procedure with unnecessary trauma.
Of the microorganisms, the most common agents that cause the development of cellulitis are staphylococcal and streptococcal bacteria.
Prevention of cellulitis and oral infections
The best way to avoid oral phlegmon is prevention.
- Regular visits to the dentist for professional teeth cleaning, plaque and tartar removal reduces the likelihood of caries and gum problems. Tartar causes bleeding gums, and microtraumas on the gums provide an entry point for bacteria and oral infections.
- General strengthening of the immune system, taking vitamins, and a varied diet with plenty of protein and fiber leave little chance for infections to enter the body through the oral cavity.
Which areas are most often affected by phlegmon?
Compared to an abscess, phlegmon has no definite boundaries. It can spread not only in the oral cavity and maxillofacial part of the face, but also spread to the neck, cheekbones, temples, and under the eyes. The most common locations are the area under the tongue, including the root of the tongue, the area of the lower jaw and chin, or both at the same time.
Good to know! The rate of spread of phlegmon can be very rapid. In 2-3 days, the inflammatory process can not only spread to nearby areas, but also change the serous form to a purulent one and cause necrotic changes in the affected areas.
Why is dental phlegmon dangerous?
Tooth phlegmon leads to serious consequences for the body. Among its complications are meningitis, phlebitis, sepsis, asphyxia and respiratory failure, and chest inflammation. In severe cases, the disease can lead a person to a wheelchair and even death.
We must not forget that the presence of an advanced disease in the oral cavity can at any time provoke a massive proliferation of microorganisms and intoxication of internal organs. It is important not only to stop this process and carry out treatment on time, but not to prevent it by contacting the dentist in a timely manner. That is why in no case should the manifestations of phlegmon be ignored; it is necessary to consult a doctor in time and cure the pathology.