Symptoms
The following possible directions of tooth displacement are distinguished:
- vertical;
- medial slope;
- distal tilt;
- tilt in the lingual (palatal) direction;
- tilt in the vestibular direction;
- combined movement.
The clinical picture depends on the topography and size of the defect.
With a defect caused by the loss of the main and lateral antagonists, a change in the position of the tooth in the vertical direction is most often observed. A tooth devoid of antagonists appears to be part of a dental defect; the distance between its occlusal surface and the alveolar process of the toothless area of the opposite jaw decreases or the teeth touch the mucous membrane. In cases where multiple teeth are removed, two, three or even four teeth may become displaced.
Deformation of the dental system in an adult develops gradually after tooth extraction, and in children and adolescents - much faster. It does not bother the patient, but is diagnosed by a doctor when examining the teeth in a state of central occlusion. In later stages of this type of deformation, teeth devoid of antagonists can be displaced to the mucous membrane of the opposite jaw. As a result of chronic microtrauma, compression restructuring of the mucous membrane develops, clinically manifested by a topographically changed configuration of the relief of the edentulous area of the alveolar process. Chronic trauma can lead to malignancy of the mucous membrane in the area of injury. The symptoms of such deformities are not limited to this sign.
A symptom of dental deformation after the loss of antagonists is blocking of movements of the lower jaw in the sagittal direction, caused by a violation of occlusal relationships. Thus, when the upper third molar is removed, the lower third molar may move upward and block the anterior movements of the lower jaw. This blocking of jaw movements over time can cause changes in the temporomandibular joint, accompanied by pain in one or both joints. Pain in the joint occurs when a defect is replaced with prostheses without eliminating the Popov-Godon phenomenon.
At the time of examination of the dentition with a half-open mouth, varying degrees of deformation of the occlusal curve are clearly determined: the teeth of the upper jaw fall below it, and the teeth of the lower jaw rise above it. When examining the periodontium of displaced teeth and the alveolar process, a different clinical picture of their restructuring can be revealed: in some cases, the gingival groove is not changed, there is no visible atrophy of bone tissue, in other cases - visible atrophy, the presence of gingival pockets and pathological mobility of teeth, the alveolar process increased in volume or unchanged.
Based on an analysis of the clinical manifestations of the Popov-Godon phenomenon, V. A. Ponomareva identifies two main forms of pathology. The first form is characterized by the fact that, simultaneously with the displacement of the tooth, there is a visible increase in the alveolar process, but there is no exposure of the tooth root and the formation of a gum pocket. The relationship between the extra- and interalveolar parts of the teeth remains unchanged.
In the second form, tooth displacement is accompanied by the phenomenon of periodontal tissue atrophy and exposure of root cement. In the second form, two subgroups are distinguished. The first subgroup is characterized by a visible increase in the alveolar process with insignificant periodontal resorption, within 1/4. In the second subgroup, there is no increase in the alveolar process; resorption of periodontal tissues at the level of half or more.
Thus, to make a diagnosis of partial secondary adentia complicated by the Popov-Godon phenomenon, the following criteria can be accepted.
- Main manifestations: partial absence of teeth;
- violation of the occlusal curve (infra- or supra-occlusal position of the tooth or teeth);
- no reduction (decrease) in occlusal height;
- a decrease in the distance (or its complete absence) between the occlusal surface of the displaced tooth and the alveolar process of the opposite jaw.
- increase in the volume of the alveolar process;
Classification of manifestations according to Ponomareva
Based on research materials on the symptoms of Popov-Godon syndrome, V. A. Ponomareva identified two forms of the phenomenon.
One stands out in that, in addition to the displacement of the dental unit, a noticeable increase in the alveolar process is formed, although the tooth root is not exposed and a gingival pocket is not formed.
The second form involves dental displacement, accompanied by necrosis of periodontal matter and exposure of root cement. It includes two subgroups.
In the first, an increase in the alveolar process is noted if periodontal resorption is insignificant. In the other subgroup, a similar phenomenon is not observed; resorption of periodontal tissues is located at a level of at least half the size of the root.
Certain signs allow diagnosing partial adentia, aggravated by Popov-Godon syndrome.
- fragmented tooth loss;
- modifications of the occlusal surface;
- no decrease in occlusion height is observed;
- reduction of the distance (or absence) from the occlusion surface of the displaced link to the alveolar process of the opposite jaw.
- increase in the size of the alveolar process;
- the presence or absence of amphodont resorption of displaced elements;
- unchanged structure of hard tissues and periodontium of natural teeth.
Treatment
Treatment of partial secondary adentia , complicated by deformation of the dentition, is carried out sequentially: first, the deformations are eliminated, and then the defects in the dentition are replaced.
Elimination of deformity is carried out using various methods depending on the type, degree and form of clinical manifestation. In order to normalize the occlusal surface and create correct occlusal relationships during subsequent prosthetics, the following is used:
- method of grinding hard tissues of displaced teeth;
- sequential disocclusion method;
- hardware-surgical - a combination of the method of sequential disocclusion with preliminary corticotomy;
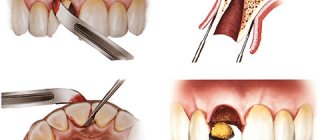
- surgical method - removal of displaced teeth.
Grinding method
This method is used to treat people over 35-40 years old when the teeth are displaced beyond the prosthetic plane by no more than half the vertical size of the tooth(s). Indications are the second form of the Popov-Godon phenomenon, the unsuccessful use of the disocclusion method.
To determine the degree of grinding, diagnostic models or lateral extraoral x-rays, as well as lateral teleradiographs, are studied. Having drawn the occlusal plane, it is determined how much the tooth has moved beyond it: the amount of tissue removed along the occlusal surface depends on this. On radiographs, the position of the line determines the indication for depulpation if the line crosses the tooth cavity.
If the displacement occurs by a small amount, then it is enough to grind off the tissue within the enamel. After this, it is necessary to conduct a course of fluoride therapy. If, during grinding, it is necessary to remove part of the dentin, then the tooth must be covered with a crown.
Disocclusion method
The method is indicated for the first form of the Popov-Hodon phenomenon in persons no older than 35-40 years. It is based on creating an intermittent action of increased pressure on the teeth involved in the process using a therapeutic removable denture with support-retaining clasps.
The treatment device is a plate or clasp prosthesis with a bite platform, and n-tagonizing with displaced teeth and uncoupling the bite in other parts of the dentition. When teeth devoid of antagonists are closed with the bite pad, the height of the lower part of the face is set for each case individually, based on the fact that the gap between the antagonistic natural teeth should be no more than 2 mm.
The action of the treatment device (uncoupling plate) continues until the natural dentition comes into contact.
The primary disocclusion of natural dentition by 2 mm after reconstruction of the dentoalveolar system does not always lead to complete alignment of the occlusal surface in the area of teeth devoid of antagonists. Therefore, the treatment process is carried out in separate stages. They proceed to the second stage of treatment when the device ceases to function due to the establishment of contact between the teeth, and the shape of the occlusal surface is not yet sufficiently aligned and the displacement of the teeth has not been completely eliminated.
The second stage of treatment consists of adding a new layer of plastic 1-2 mm thick onto the bite pad with quick-hardening plastic. The layer of applied plastic should ensure separation of natural teeth by no more than 2 mm. The occlusal relationship of the teeth is adjusted in this way until tooth displacement is completely eliminated. After leveling the occlusal surface of the dentition, the defect in the dentition of the opposite jaw is replaced with a prosthesis, depending on the indications.
When comparing removable and fixed designs of medical devices, preference should be given to removable dentures.
Since, with a significant degree of displacement of teeth devoid of antagonists, the deformation is eliminated in several stages, sequential build-up of the bite pad plastic is optimal only with a removable appliance. In addition, the removable appliance allows you to correctly establish contact with displaced teeth and correct the bite pad in a direction favorable for the movement of displaced teeth. The removable design of the device allows the patient himself to carry out hygienic treatment of the oral cavity and the medical device, and the doctor to systematically monitor the progress of the restructuring of the dentoalveolar system.
The process of restructuring bone structures when using a medical device occurs not only in the bones of the jaw whose teeth have lost antagonists, but also in the area of the defect in the dentition of the opposing jaw, as well as in the alveolar process of the upper jaw and the alveolar part of the lower jaw in the area of separated teeth. The latter gradually come closer together during treatment due to an increase in the vertical dimensions of the jaws. As a result, at the end of treatment there is a slight decrease in the incisal overlap. The latter determines the need for systematic monitoring of the incisal overlap during treatment. If it remains minimal, the design of the treatment apparatus should be changed to prevent an increase in the size of the alveolar islands in the antagonist teeth. The restructuring process is most intense in the area of the alveolar processes of displaced teeth.
Alignment of the occlusal cavity occurs due to the restructuring of bone tissue, and not due to immersion, the introduction of displaced teeth. The size of the clinical crown does not change, and the volume of the alveolar process is significantly reduced. The restructuring of bone tissue is based on the processes of regrouping the bone trabeculae of the spongy substance in accordance with the direction of the masticatory pressure forces, their zonal thinning and reduction in their number.
The phenomena of atrophy occur against the background of active renewal of bone structures, i.e., the process of bone formation is not inhibited. The duration of treatment is individual and depends not only on the degree of deformation, but also on the number of displaced teeth, the periodontal condition of the teeth of the opposite jaw and especially the age of the patient.
Hardware-surgical method
If an inflammatory reaction develops in displaced teeth and there are no signs of restructuring in the alveolar process after 3-4 weeks of treatment, it becomes necessary to switch to other methods. These methods include hardware-surgical. It can be used only in the first form of the Popov-Godon phenomenon and in the absence of contraindications to surgical interventions.
The method consists of performing a partial compact osteotomy and using a therapeutic device for disocclusion. Partial compact osteotomy (corticotomy) is performed under local anesthesia. After making a U-shaped or angular incision, departing 0.5 cm from the gingival edge of the displaced teeth, the mucoperiosteal flap is folded back. The compact plate is perforated with burs from the vestibular and palatal sides in the shape of the letter P. The transverse corticotomy line is located above (for maxillary teeth) the projection of the root apexes. It is permissible to apply several loosening holes on the palatal side over the entire area of the root projections. Sutures are applied in the usual way and further treatment of the patient is carried out according to the rules for managing a patient during surgery on the alveolar process.
Surgical method
Tooth extraction as a method of correcting deformities is used in the second form of the phenomenon and a significant violation of the occlusal plane, significant tooth mobility, and chronic periapical processes that cannot be treated.
In cases of severe hypertrophy of the alveolar process, when the considered methods have not yielded results or are not indicated, not only tooth extraction is used, but also partial resection of the alveolar process and the tubercle of the upper jaw. The level of resection is determined by the location of the maxillary (maxillary) sinus, so lateral x-rays of the sinus must be obtained before surgery. This will determine the extent of surgical intervention.
Classification
According to the classification of V. A. Ponomareva, there are 2 stages of the Popov-Godon phenomenon:
- The first is characterized by dentoalveolar elongation (an increase in the height of the alveolar ridge). In this case, there are no gum pockets and the root parts are not exposed. Periodontal resorption does not exceed 1⁄4.
- In the 2nd form, the roots are exposed, periodontal resorption is at least half the height. But the dentoalveolar elongation is not increased compared to the first form.
Pathogenesis
Histologically it has been established that in teeth devoid of antagonists, the periodontal gap is significantly narrower than in teeth with antagonists.
Statistical data show that in functioning teeth there is no difference between the width of this gap on the vestibular and lingual sides. At the same time, it has been absolutely reliably established that there is a significant difference in the width of the periodontium between the cervical, middle and apical thirds on both the vestibular and lingual sides.
In the periodontal tissue of teeth devoid of antagonists, the number of fibrous bundles is less than in teeth with antagonists, and the fibrous bundles themselves are less powerful. The predominant direction of such bundles in teeth devoid of antagonists is more oblique than in the control, or longitudinal. In the compact plate of the alveolar walls facing the periodontium, and in the ridge of the alveolar walls of teeth without antagonists, the fibrous bone has greater layering than in teeth with antagonists.
Spongiosa in teeth devoid of antagonists is constructed primarily from thinned bone beams that are in the process of restructuring. In teeth that have antagonists, spongiosis is formed by powerful beams located radially in relation to the root.
In the first form of dentoalveolar deformation, the shape of the periodontal gap is preserved in the cervical part of the root, like that of a functioning tooth, but its size decreases, and in the apical part it changes and becomes equal in size and shape to the periodontal gap in the middle part of the root, i.e., it narrows.
In the second form of dentoalveolar deformation, the shape of the periodontal fissure is preserved in the cervical and apical parts of the root on the palatal side, and its value is less than in functioning teeth and greater than in the first form of deformation. On the vestibular side, the shape of the gap changes, and its dimensions in the middle and apical parts are equal. Comparing the size and shape of the periodontal fissure, it can be assumed that in teeth devoid of antagonists, the amplitude of movement in the alveoli significantly decreases and the direction of their movement changes. If we compare the morphological data for deformities of the first and second forms, we can be convinced that with the second form of deformation the periodontal gap is wider. The processes of new formation of fibrous bone in the compact part of the alveolar wall predominate in the first form of deformation. The processes of restructuring of the spongy substance, characterized by thinning of the bone beams and a change in their location compared to the norm, are expressed to varying degrees in deformation of both forms. Thus, with deformation of the second form, the thinning of the bone beams reaches a greater magnitude and is found in a larger number of bone beams.
It can be assumed that the types of deformities observed in the clinic are based on a single process of bone restructuring as a result of the loss of its normal functional load. The structure of the periodontium changes according to new functional conditions, and when a tooth is deprived of antagonists and falls into other functional conditions, the exchange and morphological relationships between the surrounding tissues are disrupted due to a change in function. This restructuring of periodontal tissue is adaptive in nature.
Histological studies of blocks with deformation of the first form (without exposure of the root) showed that, despite the increase in the alveolar process, there is no addition of bone substance, but only the construction of new, thinner bone beams, which is characteristic of teeth devoid of antagonists. This restructuring of the alveolar process with the rearrangement of the bone beams leads to a visible increase in its volume.
Adaptive restructuring of the dental system as a result of long-term reduced function determines the predominance of atrophic processes in the underutilized section.
Based on observations of various manifestations of deformation of the dentition as a result of the absence of antagonists, it can be established that the initial period of adaptation is expressed by the restructuring of bone tissue, especially in the apical region - an increase in newly formed tissue and displacement of the tooth beyond the occlusal plane. The later period is characterized by the predominance of the atrophic process, which is clinically manifested by the exposure of the neck and root of the displaced tooth, and the beginning of the atrophy process in the form of resorption of the ridges of the alveolar walls is histologically determined even with the deformation of the first form. In other words, the first form of the phenomenon gradually transforms into the second over time, and therefore, the clinical forms of manifestation are stages of adaptive restructuring of bone tissue to change the functional load.
Histological studies of corpses of people with deformations of the dentition after the loss of antagonists, as well as experimental observations of the dynamics of bone tissue restructuring in an underloaded link, revealed a picture of adaptive restructuring under changed functional conditions in the dentofacial system.
Early reorganization of bone tissue, which underlies the deformation of the dentition, manifests itself and is accompanied by changes in metabolism. To determine early biochemical changes in jaws whose teeth have partially lost antagonists, an experimental study was conducted using radioactive tracers. A greater amount of radioactive calcium inclusion was determined on that side of the jaw where the teeth were devoid of antagonists.
It is known that the penetration of phosphorus into calcified tissue occurs the faster, the less mineralized the tissue is. Therefore, it can be assumed that radioactive calcium penetrates faster into less mineralized tissue.
Changes in calcium metabolism in an underused area of the dentition are detected by a biochemical method at an earlier time than tissue changes observed during histological examination. Functional load is the most important physiological stimulus that maintains normal mineral metabolism and the histological structure of bone tissue. Therefore, any deviation, either in the direction of increasing or decreasing the mechanical pressure on the teeth, is quickly reflected in the dynamics of the biochemical process occurring in the bone tissue of the jaws. Starting from three months after the loss of antagonists, periodontal fatty degeneration was detected, especially pronounced in cells located near the cementum of teeth devoid of antagonists.
Changed conditions after the loss of some antagonists first cause shifts in the metabolic processes of the jaws, and subsequently lead to morphological changes in both dental and periodontal tissues.
The electrical excitability of teeth devoid of antagonists is reduced - ranging from 12 to 300 μA. The decrease was more pronounced the longer the period from the moment of loss of the antagonists.
An experimental study of the nature of changes in the nerve elements of the jaws during the formation of deformation showed that in the first 3 months, along with the normal structure, hyperargeria and vacuolization were observed in some nerve fibers. In the bone marrow spaces, not only vacuolization was observed, but also fragmentation of individual nerve fibers. After 4-6 months, dystrophic changes in the nervous elements of the periodontium manifested themselves in the form of hyperargeria and cup-shaped thickening, vacuolization and fragmentation. On the part of the bone marrow spaces, a pronounced disintegration of nerve fibers into fragments and their vacuolization was observed.
After 11-12 months after removal of the antagonists, degenerative changes in the nerve fibers of the periodontium and bone marrow spaces were more significant. In the bundle of periodontal nerve fibers, decay and swelling were observed in almost all fibers. Only a few nerve fibers had a normal structure.
These histological studies and studies of metabolic processes indicate the presence of vicarious (adaptive) processes occurring in periodontal tissues in response to the elimination of chewing pressure on the tooth and its periodontal tissues. The term “atrophy from inactivity” is also used in these cases - it develops as a result of a long-term decrease in the functional load on the teeth.
Tensometric studies have established that during the chewing process, the bone tissue of the jaws is under double influence: the general functional stress state and the functional stress in the walls of the alveoli.
Thus, when the second molar is loaded, elastic deformation occurs in its periodontium. The same deformation, but of a different sign and smaller magnitude, is observed in the group of molars on the opposite side. The distribution of deformation is also observed in the presence of defects in the dentition. In the area of teeth devoid of antagonists, general functional tension is maintained and there is no tension from local influence. This, in turn, leads to a change in the nature of the deformation: instead of cyclical alternating deformations of compression and tension, mainly tensile deformation remains. This may explain not only the change in the position of the bone crossbars, but also the predominance of the resorption process over the process of bone tissue formation.
The study of elastic deformations of the bone tissue of the jaws makes it possible to confirm and clarify the mechanism of tooth movement described by Godon during the loss of part of the teeth, including the loss of antagonists.
Based on the correct position that the dental system is a single whole, Hodon considered the possibility of the existence of stability of this system while maintaining the continuity of the dentition. Each tooth has contact with the adjacent one and when loaded, its pressure is transmitted throughout the entire dentition. Hodon presented the relationship of the tooth with the antagonist and the one standing next to it at the moment of functional load in the form of a parallelogram of forces. When even one tooth is lost, the direction of forces on the teeth bordering the defect changes. Thus, when an antagonist is lost, the tooth does not experience any load coming from it, and the action of forces from neighboring teeth seems to stimulate movement beyond the occlusal curve. The absence of direct load and the action of lateral forces stimulate the process of bone formation in the periapical region and a change in the course of the bone trabeculae.
The processes of bone tissue restructuring, as a rule, proceed slowly, since general functional elastic deformations are retained during chewing and an adaptive reaction develops aimed at preserving periodontal function. Over time, the adaptive reaction fails, which is manifested by the development of the second form of the Popov-Godon phenomenon.
Tartar deposition also plays a significant role in the pathogenesis of the phenomenon, since the process of tooth cleansing is difficult due to the lack of movement of the food bolus. Tartar deposition aggravates the process of resorption of marginal periodontal tissues.
As a result of edentia and the severity of the phenomenon, depending on the time of tooth loss and their number, a change occurs in the muscular system, manifested primarily by an asymmetry of tone and contractile force.
On the deformation side, the function of the masticatory muscles changes. These changes are expressed in a weakening of muscle tension and an increase in the chewing period. On myograms this is manifested by a sharp decrease in the amplitude of the waves and a change in their character. A small amplitude of the teeth indicates weak muscle tension. Steep ascents and descents of curves reflect rapid changes in muscle tension. The difference in the nature of the teeth reflects arrhythmic muscle tension. The chewing time of an almond kernel is extended from 37 to 63 seconds.
Diagnostics
Differential diagnosis. Partial secondary adentia, complicated by the Popov-Godon phenomenon, should be differentiated:
- from partial adentia, complicated by a decrease in occlusal height and distal displacement of the lower jaw;
- from partial adentia, complicated by pathological abrasion of hard dental tissues and a decrease in occlusal height;
- from partial edentulism of both jaws, when not a single pair of opposing teeth has been preserved.
To distinguish the Popov-Hodon phenomenon from these forms of partial edentia and complications, it is necessary to examine the relationship of the dentition in the position of the lower jaw in a state of physiological rest. To do this, after determining the central relationship of the jaws, the diagnostic models are fixed in the occluder and the severity of the occlusal curve is examined both in the anterior section and in the area of the chewing teeth, the amount of space between the teeth devoid of antagonists and the alveolar process of the edentulous area.
With the central relationship of the jaws correctly fixed and the height of the lower part of the face restored, teeth devoid of antagonists do not take the place of missing teeth. In addition, the absence of displacement of teeth beyond the prosthetic plane and deformation of the occlusal curve, the normal distance between the teeth and the toothless area of the alveolar process allow us to deny the presence of the phenomenon and talk about one of the listed forms of complications with partial edentia.
Sometimes in everyday practice, these complications are mistaken for the Popov-Godon phenomenon, since when the jaws are arbitrarily closed, without taking into account the height of the lower part of the face, a false impression is created that the teeth, devoid of antagonists, have shifted into a defect in the dentition of the opposite jaw.
In the process of making a differential diagnosis, one should remember about the possible combination of the Popov-Godon phenomenon with other diseases of the dental system. For example, as a result of the loss of all chewing teeth in the lower jaw, the following complications can simultaneously develop: deformation of the occlusal curve, decreased occlusal height and distal displacement of the lower jaw.
In this case, after restoring the height of the lower part of the face and the central relationship of the jaws using wax bases with occlusal ridges both in the mouth and on diagnostic models, the degree of tooth displacement towards the defect is significantly reduced. A similar situation arises in the second and third cases of the listed complications with partial edentia.
Consequently, the presence or absence of the Popov-Hodon phenomenon, the degree of deformation of the occlusal surface (curve) can only be established after a clear determination of the central relationship of the jaws.
Preventive actions
The most effective prevention of the Popov-Godon phenomenon is to avoid situations that lead to tooth loss.
The main preventive measures include:
- proper oral care;
- getting rid of bad habits, primarily smoking;
- avoiding periodontal overload (avoiding too hard foods);
- use of sports mouthguards when playing sports;
- regular visits to the doctor.
If it was not possible to avoid tooth loss, it is necessary to replace them as quickly as possible with bridges, removable dentures or implants with a crown.
The video provides additional information on the topic of the article.