- Treatment of pulpitis surgically
- Devital amputation is
- Stages of devital amputation
- Vital amputation
- Features of devital amputation
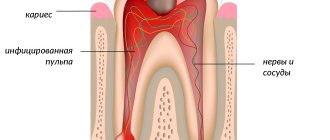
Caries is a rather insidious dental disease. If treatment is not started in a timely manner, the root canal is affected, and subsequently the pulp (connective tissue of the tooth). Modern dentistry has the ability to treat pulpitis, but in advanced cases radical measures are often required. Devital pulp amputation in children is performed in cases where preservation of connective tissue can lead to serious complications.
Pulp - what is it...
Pulp refers to the soft tissue of the dental cavity. It consists of nerve, vascular and lymphatic endings. The pulp is the main center for supplying the tooth with necessary substances and is considered a very complex organ. As long as there is pulp inside the tooth, it is considered alive. To put it simply, the pulp is a nerve. Nerve amputation is most often performed on children. At this age, the roots have not yet fully grown. In general, the chance of successful dental treatment with amputation is much greater until the age of 25.
If the root canals are cleaned and the internal cavity of the crown is cleaned, the process is called extirpation. Amputation is an easier procedure compared to this method. With it, the tooth root is preserved, and only some of the pulp is removed. It is widely used for slight root curvature and minor tissue damage.
The pulp has a coronal and a root part. As a result, in case of minor damage, only the coronal part can be removed without harm. The tooth will remain healthy, its growth and development will not stop.
There are devital and vital amputations.
Vital amputation
This method is used very often today. A tooth can be cured in one visit to the doctor. The essence of the method is the mechanical removal of pulp. To do this, they give an anesthetic injection, which acts locally.
To carry out vital removal, the viability of the root part of the pulp, the absence of symptoms of the disease and the inflammatory process must be determined.
This type of amputation is very often used for treatment in children. The roots of teeth that develop have many ribbon-like tubules. They simply need to be preserved. With baby teeth, the buds of permanent teeth cannot be damaged.
This type of amputation can be performed on the roots and crowns of the teeth.
Vital amputation is indicated in case of
- If the patient has teeth whose roots are not formed.
- If the biological method was unsuccessfully applied before.
- If the patient has chronic, concremental or acute serous-purulent pulpitis.
- If the patient has traumatic pulpitis, whose coronal part is damaged.
- If the roots of permanent teeth are not fully formed.
How is vital amputation performed?
- Determining the exact disease, making a final diagnosis, deciding on a treatment method.
- Cleansing the surface of teeth from deposits and plaque.
- Conducting anesthesia (pain-relieving injection). Anesthesia is given with modern drugs, so the entire procedure is almost painless. To carry out this stage, an anesthetic and a syringe are required.
- Isolation of teeth from saliva. This is done using a rubber dam. This is a special latex scarf with special holes made for teeth. As a result of such actions, microorganisms do not enter the root canals.
- Carrying out cavity treatment for caries. The inflamed tissue from the crown is removed and plaque is cleaned. This stage requires tips and burs.
- Opening the tooth and opening the cavity. Here, root treatment is carried out using dental instruments. Tips and burs are also needed for these purposes.
- Pulp amputation using a bur. Practice has shown the importance of this stage. Correctly done amputation is a practical success. The channels are treated with medications. At this stage, an excavator and several types of burs are needed: spherical, for deep amputation and endoburs, a probe and tips.
- Stop bleeding using a special tampon.
- Application of calcium preparations to the mouths of the canals.
- Applying an insulating pad.
- Installation of a permanent filling.
After treatment, you need to monitor the condition of the pulp every 3 months for a year.
Modern approaches to the treatment of pulpitis in primary teeth in children
L.P. Kiselnikova, Doctor of Medical Sciences, Professor, Head. Department of Pediatric Therapeutic Dentistry, Moscow State Medical University
O.S.Kovylina, Ph.D., Ass. Department of Pediatric Therapeutic Dentistry, Moscow State Medical University
E.A. Savinova, Ph.D., Ass. Department of Pediatric Therapeutic Dentistry, Moscow State Medical University
T.P.Plyukhina, Ph.D., Ass. Department of Pediatric Therapeutic Dentistry, Moscow State Medical University
S.V. Goncharova, dentist. MSHI Group of Companies
The main problem in pediatric dentistry is still caries and its complications. The presence of carious teeth as a source of chronic infection contributes to allergization of the body, decreased immunity and supports diseases of other organs and systems.
Early removal of primary teeth leads to malocclusion in the child and disruption of the sequence of teeth eruption. Lack of complete chewing of food leads to problems in the functioning of the gastrointestinal tract. Speech therapy and aesthetic problems also arise, which can lead to adverse psychological consequences.
In the therapeutic practice of a pediatric dentist, the most common form of complication of caries in primary teeth is pulpitis. Living, intact dental pulp is necessary for its normal function. The therapeutic and preventive focus of pediatric therapeutic dentistry necessitates tooth-preserving treatment of pulpitis and, if possible, preservation of the entire pulp or part of it.
Dental pulp is a richly vascularized and innervated specialized loose fibrous connective tissue that fills the pulp chamber of the crown and root canal (coronal and root pulp). In the crown, the pulp forms outgrowths corresponding to the tubercles of the chewing surface - the pulp horns. The pulp performs a number of important functions:
- plastic - participates in the formation of dentin due to the activity of odontoblasts located in it;
- trophic - ensures trophism of dentin due to the vessels located in it;
- sensory - due to the presence of a small number of nerve endings;
- protective and reparative - through the production of tertiary dentin, the development of humoral and cellular reactions, inflammation (V.L. Bykov, 1998).
The pulp of primary teeth functions for a relatively short time. It goes through three periods, which correlate with the stages of development of the primary tooth.
- Stage of tooth formation (the root of the tooth is not formed) - the period of pulp growth corresponds to the development of the crown and root.
- The stage of a formed tooth, or relative physiological rest (the root has completed its development) is the period of pulp maturation, which covers the time from the completion of root development to the beginning of its resorption.
- The stage of root resorption (loosening) is a period of regression that lasts from the beginning of root resorption until tooth loss.
During the period of regression, involutive processes occur in the pulp, disruption of its functions and gradual resorption along with resorption of the tooth root.
The development of inflammation in the dental pulp is due to the anatomical and histological features of the structure of temporary teeth:
- thin enamel-dentin layers and a large pulp chamber;
- the pulp horns of primary teeth come close to the occlusal surface and are located in close proximity to the contact surfaces;
- the pulp of temporary teeth is well supplied with blood, pre-collagen fibers predominate in it, there are many cellular elements, the connective tissue stroma of the pulp is less pronounced;
- lack of a clear boundary between the coronal and root pulp in single-rooted teeth;
- wide orifices of the root canals, a wide apical foramen and a wide periodontal fissure, the presence in 50% of cases of additional communication with tissues during the growth period in the area of the root furcation.
The indicated anatomical and histological features of the structure of temporary teeth determine the following features of the course of pulpitis:
- the predominance of chronic forms in the absence of complaints from the child;
- rapid transition of inflammation to the entire pulp and periodontal tissue;
- the presence (in 50-57% of cases) of destructive changes in the periodontal tissues.
Acute forms of pulpitis are much less common than chronic forms. Mostly, pulpitis in children is detected during a preventive examination or a routine visit to the pediatric dentist.
A complete history taking, which must be carried out taking into account the presence of concomitant chronic diseases in the child and objective examination data, helps the pediatric dentist make the correct diagnosis and choose the most rational method of treatment.
For clinical diagnosis of pulpitis of primary teeth in children, survey, examination, percussion, palpation, temperature tests, and x-ray diagnostics are used. The diagnostic value of the listed methods is different and depends on the age of the child, his individual psychological characteristics, as well as on behavior in the dental office. Diagnosis of pulpitis in primary teeth is based on objective examination data and data received from parents.
Particular attention should be paid to the external examination of the patient and the condition of the regional lymph nodes. With acute diffuse pulpitis and exacerbation of chronic gangrenous pulpitis, there may be a change in the configuration of the face due to swelling of the soft tissues.
Palpation along the transitional fold in the area of the causative tooth in chronic pulpitis does not cause pain without exacerbation (if the child behaves adequately).
Percussion does not always help to identify the causative tooth, since we are dealing with a small patient and the child may indicate painful percussion of all teeth (even healthy ones). In acute diffuse pulpitis or exacerbation of its chronic forms, there may be pain due to the accumulation of exudate in the tooth cavity or periodontal reaction.
Probing the walls and bottom of a carious cavity in young children is not recommended due to the occurrence of pain and the child’s inadequate response to the examination, which casts doubt on further reliable research and successful treatment.
After adequate anesthesia, it is necessary to remove the softened dentin with an excavator and remove the overhanging edges of the enamel. It is also important to determine whether there is a connection between the carious cavity and the tooth cavity, because we need to take into account the appearance of the pulp: it may be pink, brightly hyperemic, bleeding on probing, or dirty gray in color and not bleeding. Usually, the dentist discovers the connection between the carious cavity and the tooth cavity in the places where the pulp horns are closest to each other. In chronic forms of pulpitis, the pulp is covered with pigmented, softened dentin and the message can only be detected after its removal.
Pediatric dentists usually do not conduct temperature tests and electroodontodiagnostics (EDD) in primary teeth, because temperature tests cause an inadequate reaction in a small patient, and EDI will obviously not be indicative due to the child’s age.
When collecting anamnesis, it is necessary to take into account the psycho-emotional state of the small patient, which will allow the pediatric dentist to choose the optimal treatment method.
Clinical manifestations of various forms of pulpitis in primary teeth in children are often erased, so for diagnosis it is necessary to carry out additional examination methods. The most informative method in pediatric practice is the x-ray method. In case of pulpitis of primary teeth, an X-ray examination is mandatory, since there is often a discrepancy between the clinical picture of pulp inflammation and the condition of the periodontal tissues. An X-ray image allows you to find out the stage of formation of the root of a temporary tooth, assess the depth of the carious cavity and determine the presence of communication with the pulp chamber, the relationship of the roots of a temporary tooth with the germ of a permanent tooth, and determine the presence of changes in adjacent structures and bone tissue.
In the fibrous form of chronic pulpitis of primary teeth, changes at the bifurcation on the radiograph are detected in 57% of cases (T.F. Vinogradova, 1988), and in the gangrenous form - up to 81% (A.A. Kolesov, V.V. Zhilina, 1991) . The method is painless, which is important in pediatric practice, takes little time and allows you to choose the most appropriate tactics for treating pulpitis.
Types of radiographs: intraoral contact and extraoral (contact in the lateral projection, contact in the oblique projection, panoramic and orthopantomograms).
Figure 1. – X-ray of the jaws in the second oblique projection.
A contact intraoral radiograph allows you to objectively assess the condition of the teeth in the temporary occlusion only in the lower jaw, since in the upper jaw the permanent tooth germ is superimposed on the roots of the temporary one. But with multiple caries, multiple exposures are required, which significantly increases the tissue dose and the effective equivalent dose. Another problem is the need to place the film in the oral cavity, which causes a negative reaction in unprepared children.
An extraoral contact radiograph in a lateral projection provides an image of the chewing group of teeth in the lower jaw. The tissue and effective equivalent dose are significantly lower than with contact intraoral radiographs. This is due to an increase in the distance from the X-ray tube to the object under study and the use of intensifying screens (Yu.I. Vorobyov, V.T. Truten, 1988). With this method of research in the temporary dentition, it is possible to give an objective assessment of the X-ray picture in the area of 2-3 teeth. This method does not require placing the film in the oral cavity, which facilitates contact with the child.
The method of extraoral contact radiography in an oblique projection allows you to obtain a reliable image of not only the lower dentition, but also the upper one. To study primary molars, the method of extraoral contact radiography in the second oblique projection is used. The image of the lateral sections of the jaws is obtained in full size without significant projection distortions. The method does not require manipulation of the film in the oral cavity, which facilitates contact with the child. One image provides an image of both jaws, which reduces the number of studies and reduces radiation exposure. The tissue and effective equivalent dose is 28-30 times lower than when examining the same number of teeth using intraoral contact radiography. Moreover, it becomes possible to take pictures in identical projections, which allows you to objectively monitor the dynamics of the pathological process. The method is performed using the 5D-2 dental X-ray machine, widely used in dental practice, and requires special, expensive equipment.
A panoramic radiograph provides an enlarged image of the complete dentition of the upper or lower jaw. Orthopantomography (panoramic zonography) allows you to obtain the most complete image of the entire dental system while minimizing radiation exposure to the child’s body. However, in children during the period of temporary occlusion, a panoramic photograph of the upper jaw and an orthopaptomogram of the upper teeth do not provide a detailed picture due to the overlap of the projection of the rudiments of permanent teeth on the roots of temporary ones.
Radiovisiography as a method for studying the condition of teeth has been used relatively recently. It does not require a darkroom; the computer program provides automatic differentiated dose setting for each tooth, which improves the quality of images and significantly reduces the radiation dose to the patient. One of the disadvantages of this method is the need for intraoral placement of the sensor, which is often negatively perceived by young children.
One of the modern methods for assessing changes in bone tissue is osteodensitometry. Carrying out dynamic osteodensitometry to study the density of bone tissue makes it possible to determine the degree of destruction of bone beams in various forms of pita bullets and helps the doctor choose the optimal method of treatment (L.P. Kiselnikona, M.A. Chibisova, 2003).
In Fig. Figure 2 shows an x-ray of an intact second primary molar. Dynamic osteodensitometry data at the root bifurcation within 192 cu. e. optical density.
In Fig. 3, 4, respectively, show X-ray images of chronic fibrous pulpitis of temporary molars with changes in bone tissue at the bifurcation of the roots, a decrease in osteodensitometry values from 100 to 20 cu. e. optical density.
Figure 2. – Drawing of bone tissue without changes.
Figure 3. – Changes at the bifurcation of the roots of a temporary tooth with pulpitis.
Figure 4. – Pronounced changes in bone tissue at the bifurcation of the roots of a temporary tooth with pulpitis.
Treatment of pulp inflammation in primary teeth in children
The main tasks in the treatment of pulpitis:
- eliminate the inflammatory process in the pulp and eliminate pain;
- prevent the spread of the infectious process to the periodontium;
- restore tooth function.
- in some cases, preserve and restore pulp function.
The choice of treatment method for pulpitis in children depends on the form of pulpitis, the group of the tooth, the degree of formation of the roots, the topography of the carious cavity, the degree of tooth destruction, the multiplicity and activity of the carious process.
Methods for preserving the viability of the entire pulp in temporary teeth, due to anatomical and physiological characteristics, are used extremely rarely, since they give a high percentage of complications after treatment (V.S. Ivanov, 2003).
The method of amputation (pulpotomy and deep pulpotomy) in single-rooted temporary teeth with unformed roots is in most cases impractical. It is possible that part of the infected pulp may be preserved and the infection may spread to deeper tissues, which leads to tooth extraction.
As a rule, in clinical practice, pulpitis of single-rooted teeth with unformed roots is a consequence of early carious lesions under the age of 1 year. The reactivity of the body in such children (as well as the resistance of hard tissues) is reduced, and there is no hope for the success of vital treatment methods.
There are several methods for treating pulpitis that can be widely used in the clinic for temporary teeth: pulpotomy (vital removal of coronal pulp), the method of dental amputation followed by mummification of the root pulp, pulpectomy (extirpation method).
Based on many years of clinical practice and taking into account the introduction of modern baking methods, we recommend the following algorithm for the treatment of pulpitis of primary teeth.
Table 1
| Treatment methods for pulpitis | |||
| Maintaining the viability of all or part of the pulp | Removal of pulp with loss of its viability | ||
| Complete | Partial | Partial | Complete |
| Biological method | Vital amputation | Amputation | Complete |
| 1. Indirect coating 2. Direct coating | 1. Amputation of the coronal pulp 2. High amputation | Devital amputation | 1. Vital extirpation 2. Devital extirpation |
Method of pulpotomy (vital amputation).
Indications: temporary molars, regardless of the stage of root formation, but without signs of resorption, without pronounced changes in periodontal tissues (initial densitometry values at the bifurcation are in the range of 192-128 optical density units).
The method is carried out using drugs:
- 20% formocresol solution (35% tricresol, 19% formaldehyde in 15% aqueous and glycerin solution);
- Pulpevit No. 3 - formocresol (VladMiVa);
- Krezatin, Palpak;
- glutaraldehyde (GA), Endo-ji No. 3 (VladMiVa), containing glutaraldehyde, has an antiseptic effect;
- Endo-Zhi No. 4 (VladMiVa), contains aluminum chloride, has a hemostatic effect;
- Ferrous sulfate (15.5-55%) - ViscoStat, Astringedent (Ultradent).
The pulpotomy method using a 20% solution of formocresol or Endo-Zhi liquid No. 3 (GA) is carried out as follows. After adequate anesthesia, necrotomy is performed, the pulp chamber is opened, the overhanging edges of the pulp chamber roof are removed, and the coronal pulp is amputated. After this, special attention should be paid to stopping bleeding from the mouths of the root canals. It should be remembered that remnants of coronal pulp in the pulp chamber can cause bleeding, which can only be stopped by removing them completely. If, with a correctly performed pulpotomy, the bleeding cannot be stopped, this may indicate inflammation of the root pulp. In the latter case, this treatment method is unacceptable - pulpectomy is performed.
After stopping the bleeding, a tampon moistened with a 20% solution of formocresol or Endo-Zhi liquid No. 3 (GA) is applied to the mouths of the root canals for 5 minutes. After the specified time, the tampon is removed - a so-called “scab” is formed at the site of contact of the drug with the root pulp (the pulp becomes dark brown in color). Then zinc-oxide-eugenol cement Eodent (VladMiVa) is applied to the orifices of the root canals. Next, preparations are made for a (permanent) restoration made of glass ionomer cement or compomer, and a standard crown is fixed.
It is worth dwelling on the experience of using ferrous sulfate 20% - ViscoStat (Ultradent) during pulpotomy. This drug does not belong to the group of resorcinol-formalin compounds. Consequently, when carrying out the technique, even short-term contact of drugs containing resorcinol-formalin with the child’s body is excluded. In immature molars, coronal pulp amputation and hemostasis are performed. The ostial pulp is treated with ViscoStat - iron sulfate 20% (Ultradent), which has hemostatic and antiseptic properties.
ViscoStat gel is applied for 1-3 minutes, then removed with a cotton ball, and the tooth cavity is dried. Then Eodent zinc oxide eugenol cement (VladMiVa) is applied to the canal mouths.
It is also possible to perform pulpotomy on vital molars using the drugs Pulpotek (RP) and Pulpodent (VladMiVa). After amputation of the coronal pulp and hemostasis under anesthesia, the above drugs are applied to the canal mouths in the form of a paste. Then an insulating glass ionomer lining is applied and the crown of the tooth is restored with a composite or a standard metal crown.
Method of devital amputation followed by mummification of the root pulp
Indications: pulpitis of temporary multi-rooted teeth, regardless of the stage of root formation, without signs of physiological resorption with moderate changes in periodontal tissues (initial densitometry value at the bifurcation is in the range of 128-64 cu optical density).
Treatment is carried out in three visits. On the first visit, after anesthesia and partial treatment of the carious cavity, a devitalizing paste is applied to the exposed pulp horn. To devitalize the pulp, preparations based on paraformaldehyde or trioxymethylene are used. During the second visit, the final treatment of the carious cavity is carried out, the overhanging edges of the roof of the pulp chamber are removed, the coronal pulp is amputated, and a tampon with mummifying liquid is applied to the mouths of the root canals. For this purpose, formalin-containing preparations are used, which have antiseptic and drying properties. On the third visit, the temporary bandage and tampon with mummifying liquid are removed. A resorcinol-formalin-based paste is applied to the mouths of the root canals.
Restoration of the tooth crown is carried out using various filling materials: glass ionomer cements or composites. If the crown is significantly damaged, restoration of the anatomical shape of the tooth is carried out using standard metal crowns.
Pulpectomy (vital or devital pulp extirpation) is carried out in formed temporary single-rooted teeth or molars in case of acute diffuse and chronic gangrenous pulpitis, in the presence of a weakening of the pattern of bone beams and fiberization of the cortical plate of the tooth socket on a radiograph and osteodensitometry indicators of less than 64 y, e. optical density
After trephination of the roof of the pulp chamber, it is necessary to completely remove it using a bur; the canals are processed with hand instruments to a depth of 1-2 mm less than the radiographic length of the chamber. For medicinal treatment of infected root canals, it is advisable to use Katalyugem or Alkasept (Nord-Ost) - drugs based on quaternary ammonium compounds that have a wide range of antiseptic effects and pronounced hemostatic properties (N.B. Potapova, 2005). The material for filling the canals of temporary teeth should be absorbed during resorption and not interfere with the eruption of a permanent tooth. To fill the root canals of temporary teeth, pastes with eugenol and iodoform are used: zinc oxide eugenol paste, Vitapex (Neo Dental Chemica Prod), Metapsx (META). Then X-ray control of the filling and permanent filling with glass ionomer cement or composite are carried out.
Thus, at present, there are various methods for treating pulpitis in primary teeth, which, with differentiated diagnosis, allow in the maximum possible number of cases not only to preserve the tooth in the dentition until its physiological change, but also in some cases to ensure the viability of the pulp as a physiological barrier.
published 12/12/2011 11:43 updated 09/26/2014 – Dentistry
Devital amputation
If vital removal cannot be performed, then devital amputation is resorted to. The main indications look like this:
- Stroke, heart attack and other severe pathologies.
- If you are allergic to anesthetics.
- If it is not possible to administer anesthesia.
- If before this a vital method was used, which ended unsuccessfully.
The removal method involves treating the coronal pulp with a special paste that deadens it. After this, the pulp acquires a fibrous appearance and is easy to remove from the hole. The other part of the pulp, the root, remains intact. In addition, mummification of the coronal part of the pulp occurs due to the impregnation of the soft tissue with drugs. The pulp becomes dry and takes on the appearance of a sterile cord.
It is believed that the devital method should be used extremely rarely. This kind of amputation leads to severe periodontal inflammation. It should only be used when roots are growing. When the roots finally grow, pulp excision (further cleansing of the canals) should be carried out.
Stages of devital amputation
Devital amputation is designed for 3 visits. On the first visit, the doctor conducts an examination. On the spot, he will clean the deposits on the teeth. The procedure, of course, is carried out using anesthesia. Appliqué is usually used. The next stage is preparation of the carious plane. Next, the affected dentin is removed and the entire cavity is treated with an antiseptic. By opening the pulp horns, paste is applied to the exposed nerve. As a result, she becomes irritated. At this time, the patient feels painful sensations. Therefore, the doctor often talks about the use of painkillers.
It happens that specialists use a paste with arsenic. Then the second stage should take place on the second day. If the doctor puts a paraformaldehyde composition on the tooth, then the second visit may be after 7 days. It is very important to adhere to scheduled visit times.
The second visit goes like this. The doctor removes the temporary filling and performs the preparation. Part of the pulp is promptly removed using a bur and an excavator. An obligatory stage of this visit is treating the cavity with an antiseptic. The cavity is dried and a medicinal composition is applied to the removal site. A temporary filling is again placed on the tooth.
The third appointment is scheduled after three or five days. The doctor replaces the temporary filling with a permanent one. Here he definitely carries out its restoration with a composite.
Emphasis should be placed on special pastes. In dentistry, there are a sufficient number of special pastes with antiseptic and anti-inflammatory effects. Their choice directly depends on what kind of inflammation is present in the tooth and to what extent it is complicated. For example, in order to preserve the root part of the pulp, pastes with antimicrobial, anti-inflammatory and desensitizing effects are used. In parallel, these agents should enhance the plastic ability of the pulp. To improve the effect, the doctor often prescribes antibiotics and sulfa drugs.
Let's summarize on devital removal. The stages of treatment are as follows:
- Carrying out actions to ensure accessibility to the dental cavity.
- Application of a special devitalizing composition. For the first two steps you will need artificial dentin, instruments, burs, and tips.
- Removing the filling using tools. In case of probing, bleeding and pain do not occur.
- Opening the dental cavity and amputating the pulp. Here the bur is moved in a special way: they start from the cavity of the tooth. Correct actions lead to the opening of expanded channels.
- Treatment with medications. This treatment helps to obtain a clean cavity.
- Carrying out channel processing. The stage is carried out using impregnation methods, depophoresis and electrophoresis. The result is disinfection of the canals and their inaccessibility to infections.
- Tooth restoration. A permanent filling is placed on the treated tooth.
Features of treatment
Understanding the pulp amputation procedure cannot take place without knowing the features of the procedure:
- Removal is under no circumstances used for gangrenous pulpitis and complex periodontitis.
- Pulp removal may be used during the treatment phase. There is only one indication: the patient has narrow and crooked root canals.
- At any age, two types of treatment are available: devital and vital. Elderly people can only use the second method. This treatment is largely a compromise. The root pulp of such people cannot be preserved or saved. The procedure does not make sense, just like conservative treatment.
Chronic pulpitis
Chronic pulpitis of primary teeth is usually the next stage of acute pulpitis, but can develop independently due to caries, trauma and infectious diseases. Chronic pulpitis in children is dangerous because it is almost asymptomatic. Sharp pain and deterioration in general condition are often observed only in the acute stage. In the normal course of the disease, pain is usually mild and worsens when exposed to an irritant. Experts distinguish three types of chronic pulpitis, which occur on both milk and molar teeth.
- Fibrous.
The most common and mild form of chronic pulpitis, in which the proliferation of fibrous tissue is diagnosed. Painful sensations are not expressed, but intensify with mechanical and thermal contact. The pulp may bleed slightly. - Hypertrophic.
This form of chronic pulpitis is easy to diagnose due to the pathological growth of pulp tissue. In appearance, it resembles a small ball of granulation tissue that fills most of the carious cavity. The crown part of the tooth is usually severely damaged. - Gangrenous.
The most dangerous form. This type of pulpitis is often called advanced. Gangrenous pulpitis is accompanied by pulp necrosis in the coronal and root parts. With gangrenous pulpitis, the tooth often turns gray, and due to tissue death, a characteristic bad breath occurs.
Pulp amputation in childhood
Childhood is a special case. Unfortunately, caries occurs even on baby teeth. With this factor, the pulp also becomes inflamed. The choice of pulp treatment for children depends on:
- From caries resistance.
- From the patient's condition.
- Depending on the patient's age.
- It depends on how serious the caries is.
Vital pulp amputation in children is not performed:
- If the tooth cannot be restored.
- If there is destruction of bone tissue.
- If root resorption is observed.
- If a permanent tooth comes out.
Devital amputation is not performed in children:
- If purulent pulpitis is observed.
- If there is gangrene of the pulp.
- If there are changes in bone tissue.
Children's temporary teeth are treated only with devitalizing agents that do not contain arsenic. In this composition, the active ingredient is paraformaldehyde. The product has the necessary antimicrobial and analgesic effect. Also, under its influence, the pulp is mummified and sterilized.
Based on reviews from some dentists, I would like to note the following. Pulp amputation in children is a common occurrence. Most often, the procedure is performed within the walls of government institutions. Of course, the choice of medications here is small, but it is there. In one hundred percent of cases, pulp treatment or removal is successful and without consequences.
Pulpitis of a baby tooth: is it necessary to treat?
Treatment of pulpitis in children should be carried out in any case and as soon as possible. It is unacceptable to wait for a baby tooth to fall out, stopping only the symptoms. Failure to provide assistance to a child can result in serious complications - periostitis (in common parlance - gumboil), periodontitis - inflammation of the periodontal tissues. In addition, the infectious process in the neurovascular bundle of a baby tooth can spread to a permanent tooth when it erupts.
If a long time must pass before the eruption of a permanent tooth, premature destruction of a baby tooth due to pulpitis can lead to malocclusion - displacement of healthy teeth in a row, change in their position, which will require complex orthodontic treatment in the future.
If a baby tooth with pulpitis is soon to be replaced by a permanent one, the doctor may resort to extraction. In any case, this disease should not be ignored.
Reviews
Pulp amputation was performed on my son. The procedure was carried out in two days. She literally dragged her son to the hospital. He's a terrible coward. We thought we wouldn’t survive these two days. Somehow they pulled it through. On the first visit they put me on medication. My son cried and said that his whole mouth hurt. But I didn’t trust him much. She knew she was exaggerating. On the second, everything was cleaned and a seal was put in. The doctor explained something about the pulp. I didn’t listen much, I looked at my son’s roaring eyes. Now I understand. I didn’t think, didn’t know, didn’t imagine that the nerve could be removed from children’s baby teeth.
The tooth hurt, ached obsessively and gave no rest. I delayed with caries. Plus, some kind of inflammation also formed. Somehow I made it to the doctor. I thought that everything would be done in a day, but I was wrong. I had to go to the dentist 5 times. Every day I had something cleaned, washed, cut. The doctor said that the pulp was removed from the tooth. What it is, I understood after reading the information. It turns out now my tooth is half dead. It's a pity that this is so. It's my own fault.
Sources used: