Local treatment of erosive and ulcerative lesions of the oral mucosa
S. I. Tokmakova Doctor of Medicine, Professor, Head of the Department of Therapeutic Dentistry, Altai State Medical University (Barnaul)
T. N. Ulko Ph.D., Associate Professor, Department of Therapeutic Dentistry, Altai State Medical University (Barnaul)
O. V. Bondarenko Ph.D., Associate Professor, Department of Therapeutic Dentistry, Altai State Medical University (Barnaul)
O. V. Sysoeva Candidate of Medical Sciences, Associate Professor of the Department of Therapeutic Dentistry, Altai State Medical University (Barnaul)
Among the pathological processes localized on the oral mucosa (OM) and the red border of the lips, erosive and ulcerative lesions in leukoplakia and lichen planus (LP) occupy a special place. This is due to the fact that when treating them, a practitioner often has to deal with difficulties associated with the presence in patients of a long, persistent course of these diseases with frequent relapses [1, 3, 6, 7].
Complex treatment of this pathology includes measures aimed at reducing pain, relieving inflammation and accelerating regeneration processes after the maximum possible elimination of causative factors. However, the possibility of using medication and physiotherapeutic treatment in these patients is often limited due to the presence of concomitant general somatic diseases.
The relevance of the problem is also determined by the fact that this type of lesion has a significant prevalence (in the population of Barnaul in various age groups it ranges from 2 to 28% of cases) and is classified as an optional precancer with a high incidence of malignancy [1, 3—6]. This requires oncological alertness of the doctor and increased efficiency and timeliness of treatment. The experience of using a complex ointment developed at the Moscow State Medical University (2005) for the treatment of chronic lip diseases is interesting [2].
Purpose of the study
To evaluate the clinical effectiveness of using a complex ointment in the complex treatment of erosive and ulcerative lesions of the oral mucosa with leukoplakia and lichen planus.
Material and methods
Clinical studies were carried out from 2008 to 2011 at the Department of Therapeutic Dentistry of ASMU. Under observation were 35 patients diagnosed with K.13.2 “leukoplakia” (20 people) and L.43 “lichen planus of the oral mucosa, erosive-ulcerative form” (15 people).
During the clinical examination of patients, the presence of past and concomitant diseases, bad habits, and occupational hazards was revealed during the interview process. In addition, attention was paid to allergic status and heredity. The duration of the disease, the nature of the complaints, as well as the time of onset of the first symptoms were determined. They found out whether treatment was carried out for this disease and what its effectiveness was.
Examination and palpation of the maxillofacial area included determination of color, integrity, skin turgor, condition of the skeletal and muscular system, and regional lymph nodes. When assessing the state of the oral mucosa, we paid attention to the architectonics, color, moisture, and the presence of pathological elements. The condition of periodontal tissues, teeth, the presence of dissimilar metals was determined, and traumatic factors were identified.
Dental examination of the oral mucosa was performed using a “Visioner 21A” light stomatoscope from Morita Corporation (Japan) at a magnification of 10 to 40 times. Signs of malignancy were excluded visually and by palpation; if necessary, the patient was referred to an oncologist to clarify the diagnosis.
The study of the medical history of the examined patients, the results of laboratory tests, and advisory opinions made it possible to establish the background diseases accompanying the erosive-ulcerative form of leukoplakia and PL. All patients had pathology of the gastrointestinal tract (100%) and nervous system (100%). Three patients suffered from diseases of the cardiovascular and endocrine systems (9%).
To assess the timing of pain disappearance, we used the pain index (PIB) according to the Hossli-Bergman scale. The assessment was made in points from 0 to 4 before and after treatment: no pain - 0 points, mild pain - 1 point, moderate pain - 2 points, severe pain - 3 points, unbearable pain - 4 points.
The treatment plan included sanitation of the oral cavity, professional hygiene, and elimination of traumatic factors. Patients were advised to give up bad habits: smoking, drinking alcohol, biting lips and cheeks.
After local elimination of traumatic factors, treatment of erosive and ulcerative lesions was carried out according to the following scheme:
- Application anesthesia (gel “Kamistad”, “Cholisal”, “Lidochlor”, pyromecaine ointment 5%, etc.).
- Applications of proteolytic enzymes (0.1% solution of trypsin or chymotrypsin).
- Treatment with antiseptics (0.05% chlorhexidine solution, 1% iodinol solution, herbal decoctions, etc.).
- Application of a complex ointment developed at Moscow State Medical University (2005).
Composition of complex ointment:
- Sol. Retinoli acetatis olesae - 1.0
- Sol. Tocopheroli olesae - 1.0
- Thiamini bromidi - 0.2
- Insulini acropidi - 3.0
- Ung. Celestodermi - 30.0
- Ung. Solcoseryli - 20.0
- Mf unguentum
- DS For applications to the oral mucosa.
The components included in the ointment had a complex effect on various parts of the pathogenesis of diseases. An oil solution of vitamin A, when applied topically, stimulates epithelization processes, and when taken orally, helps normalize the condition of the epithelium. A solution of tocopherol acetate is an antioxidant, promotes protein synthesis, cell proliferation and acceleration of reparative processes, and also improves neurotrophic processes. Vitamin B1 normalizes the functions of the nervous system and improves local trophism. Insulin, when applied topically, helps loosen membranes and prolongs the effect of other components of the ointment. Celistoderm has anti-inflammatory and antipruritic effects. Solcoseryl improves metabolic processes, accelerates tissue regeneration, especially with neurotrophic lesions, and also has an angioprotective effect.
results
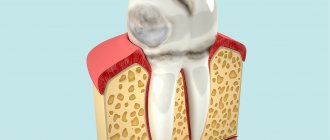
When studying the clinical picture before treatment in patients in the oral cavity, erosions and ulcers measuring from 0.5 to 2.2 cm were determined against the background of edematous, hyperemic mucosa with papules merging into a mesh pattern (43% of cases), against the background of flat foci (31% of cases). ) or verrucous leukoplakia (26%). The most common location of erosive and ulcerative lesions was the mucous membrane of the cheeks and tongue, less often the gingival margin and floor of the mouth (Fig. 1).
Rice. 1. Erosion and ulcers of the tongue with leukoplakia (before treatment).
Skin rashes characteristic of LP were present in 3 patients (20%). Dental examination revealed alternating areas of hyperemia and hyperkeratosis with epithelial defects. The surface relief of the oral mucosa was smooth or finely lumpy, keratinization of varying degrees of severity, angioarchitecture in the form of specks, stripes and loop-shaped vessels.
After a course of treatment using applications of a complex ointment, initial epithelization was observed in all patients on the 2nd day. Patients noted a decrease in pain when eating and an improvement in their general condition. After 3 days, the pain completely disappeared (Fig. 2), and after 1.5 weeks, complete epithelization of the mucous membranes was observed (Fig. 3).
Rice. 2. Epithelization of erosions and ulcers of the tongue in leukoplakia (on the 4th day of treatment). Rice. 3. Condition of the tongue 1.5 weeks after treatment of leukoplakia.
Dentoscopically, a smooth relief was noted on the oral mucosa, there was no keratinization, and the vascular architecture was presented in the form of speckles and stripes.
To increase local immunity and prevent relapses, patients were prescribed the topical immunostimulating drug Imudon, 6-8 tablets per day sublingually for 20 days.
Long-term results of treatment of patients with erosive and ulcerative lesions were monitored for 5 years. Relapses were observed after six months in 7 patients due to dietary violations and exacerbation of general somatic diseases.
Based on the above, we can conclude that the complex ointment is an effective remedy in the complex treatment of erosive forms of PL and leukoplakia of the oral mucosa and is recommended for implementation in dental practice.
- Borovsky E. V. Therapeutic dentistry / E. V. Borovsky. - M.: Medical Information Agency, 2006. - 800 p.
- Brusenina N.D. Lip diseases: Textbook / N.D. Brusenina, E.A. Rybalkina. Ed. Barera G.M. - M.: Federal State Educational Institution "VUNMC" of Roszdrav, 2005. - 184 p., ill.
- Bykova I. A. Cytological characteristics of prints of the oral mucosa using the cell differentiation index / Bykova I. A., Agadzhanyan A. A., Banchenko G. V. // Laboratory work. - 1987, No. 1. - P. 33-35.
- Vasiltsova S.V. Dental morbidity and effectiveness of therapeutic and preventive care for the population of the city of Barnaul: abstract of thesis. dis. Ph.D. honey. science / S. V. Vasiltsova. - Novosibirsk, 2005. - 24 p.
- Therapeutic dentistry: textbook: in 3 hours / Ed. G. M. Barera. - M.: GEOTAR-Media, 2005. - Part 3. - P. 195-211, 218-233.
- Therapeutic dentistry: national guide / Ed. L. A. Dmitrieva, Yu. M. Maksimovsky. - M.: GEOTAR-Media, 2009. - 912 p.
- Tokmakova S.I. Oral mucosa in elderly and senile people and its changes in visceral pathology // Dis. Dr. med. Sci. - Omsk, 2002. - 291 p.
Minimally invasive approach to the treatment of erosive loss of dental hard tissue
The loss of structural tooth tissue, as a rule, is a polyetiological disorder. Traditionally, the terms erosion, abrasion, and attrition are used to classify different forms of loss of enamel and dentin of a non-carious nature. Differential diagnosis of various forms of pathological abrasion is extremely important for choosing the most appropriate method of treating affected teeth.
In this article we will consider the pathophysiology of the loss of superficial hard dental tissues due to the patient’s gastroesophageal reflux, as well as minimally invasive methods for correcting this dental pathology.
Tooth erosion
Erosion is a physical mechanism of tissue wear caused by the frictional effect of moving fluids. Tooth erosion is identified as a disorder caused by chemical or electrolytic factors of non-bacterial origin, which in most cases involves an acid reaction. Recently, another term “biocorrosion” has appeared in the literature, implying the implementation of a mechanism of chemical, biomechanical or electrochemical action, which, in turn, causes molecular degradation of the natural properties of living tissues. Sources of acids acting on teeth can be endogenous and exogenous. The former enter the oral cavity from the stomach as a result of vomiting or gastroesophageal reflux disease (GERD), while the latter are components of diet, medications or the professional environment.
GERD
Gastroesophageal reflux disease is a chronic condition colloquially referred to as heartburn. The pathology develops due to regurgitation of gastric acid into the space of the esophagus and oral cavity. The American Gastroenterological Association published the Montreal Consensus, which defines GERD as “a condition that occurs when reflux of stomach contents causes unpleasant symptoms and/or complications.” Symptoms of GERD are divided into esophageal and extraesophageal. The prevalence of dental erosion in adult patients with GERD has been documented to be approximately 25%. Risk factors for developing GERD include alcohol and caffeine consumption, obesity, pregnancy and sleep apnea, and use of non-steroidal anti-inflammatory drugs.
Dental manifestations of GERD
Dental symptoms of GERD include tooth erosion, hypersensitivity, sour taste and bad breath, and signs of mucosal inflammation. The process of enamel dissolution begins at a pH level of about 5.2, and the pH value of stomach acid reaches 2.0. Sometimes dentists are the first to suspect that a patient has GERD, even in cases of so-called “silent reflux.” Typical dental symptoms of GERD include loss of enamel from the palatal surface of the front teeth, as well as thinning and reduction of the crown in particularly difficult cases; Crater-shaped defects may be observed in the area of the distal teeth, and the extent of damage to the lingual and occlusal surfaces of the lower teeth depends to a large extent on the position of the head. The dentin of the front teeth exposed by acid causes the effect of whiter teeth with the development of hypersensitivity symptoms. Opposing teeth often show signs of supereruption. Clinically, this limits the space for restoration of teeth on the palatal side.
Photo 1. Normal level of horizontal and vertical overlap of the anterior teeth.
Photo 2. The effect of super-eruption of the lower incisors due to abrasion of the palatal surface of the upper incisors.
During treatment, despite such conditions, it is important to maintain the vitality of the teeth, providing for this a sufficient amount of space for restoration. Methods for correcting pathological loss of hard tissue due to acids in conditions of limited space for restoration include the following: selective endodontic treatment when volumetric preparation is necessary; orthodontic reposition of anterior teeth; enameloplasty of antagonist teeth; expansion of the vertical parameters of the bite and restoration of the occlusal surfaces of the distal teeth and palatal surfaces of the anterior teeth; achieving correspondence between the position of the maximum fissure-tubercle contact (maximum intercuspidation - MIC) and the position of the central ratio (CR); production of palatal composite veneers using the Dahl technique (photo 3).
Photo 3. Diagram showing the pattern of restoration of the palatal surface of teeth using composite.
When implementing the classical approach to treatment, the doctor would have to sacrifice the vitality of the anterior teeth of the upper jaw and then cover them with crowns. Such treatment compromises the overall biomechanical prognosis of rehabilitation and reduces the actual effectiveness of iatrogenic interventions. In addition, in the area of the edges of the crowns, the risk of developing secondary caries increases, due to which the process of tooth destruction may continue. Orthodontic tooth reposition, despite its mini-invasiveness, is a time-consuming and not always financially justified procedure. Enameloplasty of antagonist teeth, despite the fact that it allows to increase the amount of space for restoration, is also characterized by the risk of developing hypersensitivity of the treated supporting units. In complex forms of pathological abrasion caused by the influence of erosion, it may be advisable to correct the vertical parameters of the bite and harmonize the ratios of MIC and CO. In this way, it is possible to increase the existing interdental space by a few millimeters for restorations. Particularly difficult to treat are localized forms of pathological abrasion with loss of hard tissue only on the palatal side of the anterior teeth and, to a small extent, in the area of the distal teeth. It is in such cases that it is advisable to apply the principles of restoration with composite veneers according to Dahl.
Clinical case
A 20-year-old patient sought dental care for uneven contours of his front teeth, which were compromising the appearance of his smile (Figure 4). He also complained of hypersensitivity, and two weeks ago he noted acute pain in the area of the 10th tooth, which had previously been treated endodontically. A broken amalgam filling was noted in the area of the 3rd tooth. Upon examination, teeth 6-11 were found to show signs of significant loss of enamel and dentin and were susceptible to moderate wear. Because of this, the patient experienced loss of the anterior insertion route (Figures 5-7).
Photo 4. View of the smile before treatment.
Photo 5. Thinning of the enamel on the labial side of the teeth and the presence of non-carious cervical lesions.
Photo 6. Signs of loss of hard dental tissues caused by erosion.
Photo 7. View of teeth with loss of enamel from the palatal side.
Considering the palatal location of the lesions of the hard tissues of the teeth, the doctor suggested that such symptoms could be caused by GERD. Analysis of general somatic history revealed that the patient suffers from heartburn symptoms at least 4 times a week. To relieve these symptoms, he used over-the-counter medications. The patient sometimes drank alcohol, but never smoked. During a detailed dental analysis, a shift in the inclination of the occlusal plane of the upper jaw, a reverse position of the smile line, a lack of visualization of the crowns of the upper incisors even in the position of lip reposition, the presence of a thin biotype of soft tissues, an asymmetrical position of the gingival contour, incorrect axial position of individual teeth, and a change in the width ratio were discovered. and the length of clinical crowns, the presence of signs of biocorrosion in the area of molars and premolars, discoloration of the 10th tooth and changes in the ratio between MIC and CV.
Treatment plan
The complexity of the treatment was that the dentist needed to restore the lost anatomy of the palatal surface of the teeth in the absence of interocclusal space. Orthodontic and endodontic treatment methods were rejected by the patient as alternatives. Thus, it was decided to carry out minimally invasive rehabilitation with veneers according to Dahl principles. This principle involves direct restoration to restore the palatal anatomy of the maxillary anterior teeth while simultaneously modifying their labial surfaces and incisal edges. The comprehensive treatment plan could be summarized as follows:
- restoration of the anatomy of the palatal and labial surfaces with a composite material with the formation of disocclusion in the area of the distal teeth during eccentric movements of the jaw;
- correction of the anterior route of administration;
- restoration of non-carious cervical defects in the area of premolars and molars;
- occlusal equilibration after restoration of distal occlusion by controlling the level of passive eruption.
Stages of treatment
First, plaster models were made. On the model of the upper jaw, wax modeling of the palatal and vestibular surfaces of the anterior teeth was carried out (photo, taking into account the lost volume of tissue and the need to minimize the effect of non-axial loads on the anterior teeth of the lower jaw. After this, an impression was taken from the wax reproduction of the teeth, from which a composite reproduction was made. The last one after bonding in the mouth, contoured and polished. The anterior occlusion was adjusted to ensure uniform contact between all teeth. The patient used the composite reproduction for 48 hours, after which an impression was taken from it. The impression was taken again from the composite reproduction after all corrections were completed allows the clinician to most accurately approach the future restoration of teeth 6-11.
On the model of the upper jaw, wax modeling of the palatal and vestibular surfaces of the anterior teeth was carried out (photo, taking into account the lost volume of tissue and the need to minimize the effect of non-axial loads on the anterior teeth of the lower jaw. After this, an impression was taken from the wax reproduction of the teeth, from which a composite reproduction was made. The last one after bonding in the mouth, contoured and polished. The anterior occlusion was adjusted to ensure uniform contact between all teeth. The patient used the composite reproduction for 48 hours, after which an impression was taken from it. The impression was taken again from the composite reproduction after all corrections were completed allows the clinician to most accurately approach the future restoration of teeth 6-11.
Photo 8. Restoring anatomy with wax.
In the area of the 9th tooth, the composite reproduction was removed and the vestibular surface was minimally prepared with a diamond bur. No preparation of the palatal surface of the tooth was performed. An ultra-thin retraction cord was placed into the gingival sulcus area (Figures 9-10). Teflon tape was used to isolate tooth 9. Then, with 37% orthophosphoric acid, total etching of the vestibular surface was carried out for 10 seconds, and the palatal surface for 5 seconds. A single-phase adhesive was applied over all tooth surfaces for 20 seconds to form an even layer of bond. A composite with a white enamel tint was introduced into a silicone key and fitted to the palatal surface of the 9th tooth.
Photo 9. Minimally invasive preparation of the 9th tooth from the vestibular side.
Photo 10. The 9th tooth was not prepared on the palatal side.
This layer was distributed evenly with optimal thickness over the entire surface (photo 11). After polymerization of this layer, dentin shade A2 was used to form a natural pattern on the tooth surface (photo 12). After polymerization, a transparent layer of composite was used to restore the cutting edge. A finishing layer of A2 enamel was used to create a more natural and full contour (photo 13).
Photo 11. Formation of a palatal composite shell from a nanofilled composite.
Photo 12. Layering of dentin shades.
Photo 13. Layering of enamel shades.
A similar restoration algorithm was implemented in the area of all affected anterior teeth of the upper jaw. The restorations were adjusted to ensure their most uniform contact in the MIC position. The anterior insertion route was modified to evenly distribute contact between the incisors during protrusive movements and the canines and incisors during lateral excursions. Finally, finishing and polishing of the restorations was carried out (photos 14-18). Erosive cervical lesions in the premolar and molar areas were restored using glass ionomer cement modified with a composite component. After 8 months, the patient underwent occlusal equilibration to correct the relationship between the MIC and the CS.
Photo 14. View of the smile after treatment.
Photo 15. View in the position of maximum intercuspidation after treatment.
Photo 16. Lateral view on the right; controlled disocclusion of distal teeth.
Photo 17. Lateral view on the left; controlled disocclusion of distal teeth.
Photo 18. View of the restored palatal surfaces of the incisors.
Additional treatment
The patient was advised to avoid eating habits that could trigger the development of reflux. Firstly, do not lie down immediately after eating a heavy meal. Secondly, to minimize the risk of developing reflux during sleep, he was advised to ensure that his head was positioned higher than the rest of his body.
Discussion
A systematic analysis of signs of pathological wear of anterior teeth is extremely important to achieve a successful result in the aesthetic and functional rehabilitation of the patient. New advances in the industry of composite materials make it possible to successfully restore areas of hard tissue loss, even in cases of severe erosive lesions caused by GERD. Of course, dental treatment in such cases can be carried out using classic crowns, but this approach requires additional endodontic intervention, which, in turn, weakens the tooth and reduces the prognosis of its biomechanical functioning. In addition, the risk of developing secondary caries similarly increases. Therefore, the physician must understand that more invasive treatment algorithms must be implemented after minimally invasive alternatives have failed. In this case, one should also pay great attention to the volume of the lesion: if the surfaces of the distal teeth are subject to severe destruction with the loss of adequate bite height parameters, then in such cases, of course, crowns cannot be avoided.
In 1975, Dahl proposed the concept of space shaping in the treatment of localized hard tissue loss in the anterior teeth. This approach involved the use of a cobalt-chrome apparatus with an anterior bite plane, which allowed deocclusion of the distal teeth. The principle of treatment was that the distal teeth thus had the conditions for more adequate eruption and the formation of the necessary occlusal relationships. Over time, the principle proposed by Dahl has changed and been modified somewhat. One of these modifications is the technique presented in this article, which made it possible to preserve the remaining hard tissues of the affected anterior teeth as much as possible.
The front teeth were restored using a nanofilled composite, which has great strength, resistance to abrasion and suitable optical properties. But, even despite this, the doctor must understand that the degree of wear of such restorations during operation will be much greater than their metal or ceramic counterparts, however, the treatment method itself is completely acceptable for young patients. With the initial restoration of the anterior teeth, it is possible to bring the distal teeth into disocclusion. With this transition, the patient may experience some speech problems associated with changes in the vertical parameters of the bite. Over time, they will be compensated for by passive eruption of the distal teeth and slight intrusion of the anterior teeth. Lack of posterior occlusal support can lead to the destruction of restorations in the anterior region and increased mobility of the anterior dentition. That is why these patients require periodic monitoring. However, it should be understood that even chips or significant wear of restorations in the area of the front teeth does not cause any harm to the teeth themselves, which can later be restored using orthopedic structures.
In patients with GERD, in addition to dental treatment, it is also important to provide general medical relief of the symptoms of the disease. If it is not possible to stop GERD or bulimia, it is still better for the patient to have classic full crowns made, which will provide better protection for the teeth. At the same time, the doctor should always remember that the opportunity to carry out the most aggressive treatment is always possible, and minimally invasive treatment is only possible first.
Conclusion
GERD is becoming an increasingly common disorder, the consequences of which significantly influence changes in dental status. In cases of so-called “silent reflux,” the dentist may be the first to diagnose GERD and then refer the patient to the appropriate specialist. Significant erosive loss of enamel causes increased flexibility and weakening of the structural integrity of the tooth, compromising its function and aesthetics. Treatment of such complications should begin with minimally invasive approaches, and in cases of ineffectiveness of the latter, move on to more extensive iatrogenic interventions.
Author: Aliasger Tunkiwala, MDS (Private Practice, India)