9426
Constant pain and discomfort in the lower jaw and temples are the first signs of pathological changes in the temporomandibular joint.
This problem is usually known to people with malocclusions. Unfortunately, it is impossible to eliminate negative symptoms with mouth guards or brace systems without additional treatment.
In such a situation, dentists recommend first performing splint therapy.
Examination and differential diagnosis
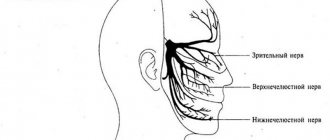
Dr. Peter Dawson once said, “Dentists are doctors of the masticatory system.” Every day, doctors carry out interventions in the area of the dentofacial apparatus, correcting the function of the TMJ, masticatory muscles, occlusion, trigeminal nerve system and even the central nervous system (Fig. 1). Disharmony, dysfunction and deformation of the dental system manifests itself in a variety of symptoms, so a thorough examination of the dental status is critical for the planning and implementation of the future treatment protocol, as well as the differential diagnosis phase (Fig. 2).
Rice. 1.
Rice. 2
A systematic approach to examining a patient involves identifying one of three main types of dental disorders:
- Extracapsular: problems of the masticatory system without damage to joint structures.
- Intracapsular: the presence of lesions in the structure of the TMJ.
- Others: general somatic disorders that affect the condition of the dentofacial apparatus; therefore, the treatment process involves the participation of additional specialists (Fig. 3).
Rice. 3
During the examination, it is necessary to ask the patient several questions, for example: “Where do you think the cause of the discomfort lies?” - after all, etiological factors are variable and may include the following:
- pain in the cervical spine;
- somatic pain, which can be triggered by fibromyalgia, chronic fatigue syndrome or rheumatoid arthritis;
- radiating pain as a result of reflex sympathetic dystrophy or chronic regional pain syndrome;
- central neurological, pathological, vascular, migratory or other lesions;
- trigeminal neuralgia with peripheral symptoms.
But, as you noticed, all these questions relate to the need to confirm or, conversely, exclude the presence of so-called other causes of occlusal pathology. Depending on the causative general somatic diagnosis, the use of a splint may be indicated, but may also be contraindicated.
The next question the doctor should ask the patient is: “Does it seem to you that the cause of the disorder is in the joint?” If so, it is very important to determine the diagnosis of articular pathology according to the Piper classification. Intracapsular disorders usually present with disc displacement (partial or complete) with the potential for osteoarthritis, but can also be caused by rheumatoid arthritis or osteoma. Treatment options also directly depend on the diagnosis. To diagnose the condition of the joint, tomography, computer or magnetic resonance imaging methods can be used. Treatment should begin only after a final diagnosis has been made. The patient should also be asked about masticatory muscle problems and occlusion. Occlusal-muscular pathology without affecting the joint area can be corrected through splint therapy, but the doctor must clearly understand which muscle and where should be deprogrammed in order to ensure an adequate pattern of movements of the lower jaw. In order to determine muscle soreness and the state of their hyperfunction, you can palpate the diagnosed area.
During the diagnosis, the doctor should remember the following aspects:
- Clenchers typically experience soreness in the temporal and masticatory muscles.
- The chronic protrusive position of the lower jaw provokes the development of pain in the area of the lateral pterygoid muscles and the anterior neck muscles.
- When registering Hit-and-slide occlusion (transition of the central relation to the state of maximum fissure-tubercle contact), clenchers and bruxists experience pain on palpation of all the above-mentioned muscles (Fig. 4-5).
Rice. 4. Problems begin with a mismatch between the central authority and the central authority.
Rice. 5. When shifting from the CO position to the CO position, muscle incoordination may occur.
Rice. 6. Permissive splint with anterior median contact point and nociceptive trigeminal inhibition function
It has also been found that tension in the temporal muscles often provokes the development of headaches and pain stimulus, which, in turn, triggers a number of vascular changes responsible for the progression of migraines.
Advantages and disadvantages
This technology has a number of undeniable advantages that make it actively in demand. These include:
- wide range of uses - the number of pathologies that can be eliminated using splint therapy is quite large;
- ease of use - occlusal splints do not cause any particular discomfort while wearing, due to their softness and elasticity;
- the ability to adjust the wearing time - if necessary, the patient can remove them for a while;
- the therapeutic effect (disappearance of pain) occurs within a short time;
- a positive result occurs in the vast majority of cases.
Attention! Splint therapy is indispensable for TMJ diseases if other methods have failed.
As for the shortcomings, there are few of them, and they are relative. The disadvantages of the method are:
- long treatment period - the final result is visible only after a few months;
- high price.
Disadvantages also include the likelihood of individual intolerance to the splint being in the oral cavity. But the risk of its occurrence is no higher than that of other treatment methods.
Occlusal splints
The two main types of occlusal splints are permissive (permissive) and directive (directive). Permissive splints are formed in such a way as to eliminate painful occlusal contacts and normalize the condition of the masticatory system. The primary task of such splints is to change the occlusion and achieve complete seating of the articular head under the control of the masticatory muscles. Such tires are mainly represented by designs with a horizontal plane. Classic permissive splint designs are those with anterior midpoint contact and full contact. Permissive splints with an anterior midline contact point are designed to separate all teeth except the incisors.
The purpose of their use is as follows:
- Elimination of interfering occlusal contacts to ensure complete seating of the articular head.
- Providing freedom of movement for jaw positioning by eliminating contraction of the masticatory muscles.
- Ensuring free function of the lateral pterygoid muscle and anterior neck muscles when closing the oral cavity.
Using the electromyography method, it has been shown that contact in the molar area allows for 100% of the clamping force, while contact only in the premolar area is 60% of the maximum biting force, and in the area of the incisors only the muscles that lift the mandible can develop only up to 20-30% of the maximum possible jaw compression force. The width of the platform of the median contact point is limited by the width of the 2 lower incisors, which in millimeters is from 8 to 10 mm. Eliminating contact between distal teeth reduces the painful factor that provokes the sensory response. Such a mechanism, through the system of trigeminal interaction, makes it possible to free a person from vascular changes inside the skull, roughly speaking, to free him from headaches and migraines, if the development of such was associated with occlusion disorders. For this purpose, special splints for nociceptive trigeminal inhibition (NTI) are used. Other types of splints with an anterior midline contact point are the Luciajig (GreatLakesOrthodontics, LTD, Tonawanda, NY) (Figure 7) and the B-splint (Figure 8).
Fig.7. Permissive splint with anterior medial contact point Luciajig
Rice. 8. Permissive splint with an anterior median contact point of the B-splint type (for bruxism)
Permissive full contact splints are used to recreate ideal occlusion (Fig. 9). The contacts are formed so as to be evenly distributed over all teeth with full positioning of the joint by the muscles that lift the mandible, or directly by the doctor’s hands. The bimanual Dawson technique is used to seat the joint when the jaw occlusion is adjusted into centric relation by means of a splint (Fig. 10). It is extremely important to ensure adequate joint position when correcting the working position of the mandible. Only with this approach can the maximum therapeutic effect be achieved from the use of a permissive full contact splint.
Rice. 9. Permissive splint with full contact on the lower jaw
Rice. 10. Bimanual Dawson Deprogramming Technique
During excursive movements of the jaw, only the front teeth come into contact, thus reducing the activity of the masticatory muscles. The smooth, flat cusp-to-cusp contacts that form on the splint are designed to provide anterior guidance, which in turn allows freedom of lateral movement, as well as immediate disocclusion of all distal teeth.
Advantages of permissive full contact tires:
- elimination of discrepancies between the proper position of the joint and the established occlusion (CO = MIC);
- increasing the area to distribute the bite force;
- reducing the load on the joint;
- achieving adequate functional occlusion;
- the ability to monitor the stable state of the occlusion and joint.
Permissive full contact splints can be made for both the upper and lower jaws (Fig. 11). Splints on the lower jaw are characterized by certain advantages for practicing doctors :
- Reducing the effect of speech impairment (compared to maxillary splints).
- Less visualization when speaking.
- Possibility of forming deeper retention elements.
- Minimizing the effect of postoperative tooth sensitivity when forming retention elements only on the lingual side.
- Possibility of using splints both during the day and at night.
Rice. 11. Permissive splint with full contact on the upper jaw
Guide elements allow you to adjust the position of the joint so as to remove it from the position that provokes painful symptoms. That is, permissive splints allow the maximum anterosuperior position of the articular head to be achieved under the action of the levator mandibular muscles, while directive splints correct the position of the mandible in the anterior direction based on the design of the splint and excluding the achievement of a centric relation state. Anterior guide splints are used in two cases: for complex joint trauma with swelling of the retrodiscal space and for chronic painful disc displacement (Fig. 12).
Rice. 12. Front repositioning guide splint
The essence of the technique
TMJ dysfunction is a disease of the temporomandibular joint, expressed in pathological changes in the functions of its muscles and ligaments, disruption of the relative position of joint elements and changes in occlusion.
According to statistics, up to 70% of dental patients have some form of TMJ dysfunction. The disease manifests itself as clicking and crunching in the joint, jaw and/or headache, tinnitus, limited jaw mobility (difficulty opening the mouth), bruxism and some other symptoms.
A splint, or otherwise occlusal splint, is a mouthguard made of elastic polymers (silicone, acrylic and other materials). Thanks to its special shape, when worn for a long time, the hypertonicity of the masticatory muscles is relieved, the TMJ ligaments are stretched, and the occlusal load is normalized.
As a result, pathological symptoms disappear - crunching and clicking in the joint, pain, speech impairment, distortion of the facial profile, bruxism.
Severe trauma with swelling of the retrodiscal space
In cases of acute injury with swelling of the soft tissue behind the condyle, it is advisable to hold the articular head anteriorly to avoid compression of the affected retrodiscal space. Dr. Parker Mahan, former chairman of the University of Florida Facial Pain Center, even coined the phrase “Cheerleader Syndrome” to describe a clinic of cheerleaders who fell on their chins, causing them to develop joint pain, retroarticular swelling, and acute distal open bites. Examples of such symptoms are also “Airbag Syndrome”, “Barriff Syndrome” and “Extreme Gaming Syndrome”. In such cases, displacement of the articular head anteriorly for a period of 10-14 days is a diagnostic measure, as a result of which it is possible to achieve decompression of the already swollen and painful tissues. This treatment algorithm is also accompanied by an appropriate diet, taking anti-inflammatory drugs and physiotherapeutic procedures.
Chronic painful disorders associated with disc displacement
If anterior displacement of the disc causes compression of the retrodiscal space, it is logical that displacement of the condyle to a more anterior position can only have a positive effect. If it is possible to achieve complete reduction of the disc in the anterior joint position using a guide splint and the proper position cannot be achieved using a permissive splint, the choice between these designs is clear. The challenge is to ensure long-term stability of the required disc position. But in general it seems impossible to achieve a healthy anterior position of the disc and head and then carefully move it to the desired superior position in the fossa. In addition, fibrous contractures of the lateral pterygoid muscle, unstable formation of soft tissues in the joint structure and destabilized bite remain a problem.
Indications and restrictions
Splint therapy is indicated for the following pathological manifestations:
- discomfort or pain when chewing;
- crunching and clicking when opening/closing the mouth;
- limitation of NP mobility;
- bruxism;
- rapid fatigue of the LF muscles when chewing and talking (manifests mainly at the end of the day);
- headache.
Splints are also used in the diagnosis and treatment of a number of pathologies - periodontal disease, periodontitis, stress syndrome, myofascial syndrome, etc. In some cases, wearing occlusal splints is indicated when installing prostheses and orthodontic devices - as a means of adaptation.
Important. Splint therapy is effective only against TMJ dysfunction, that is, disorders that do not affect the morphological structure of the joint components. Occlusive splints are not intended for the treatment of systemic articular diseases such as arthritis and arthrosis.
A contraindication to splint therapy is inflammation in the RP, as well as pathologies that are caused not by a violation of occlusion, but by some other factors.
Treatment Options
Patients experience the following manifestations of simple occlusal-muscular disorders:
- Minimal symptoms (teeth wear, mobility and change in position of teeth, muscle soreness on palpation).
- Occlusal instability and uncoordinated muscle activity in states of central ratio (CR) and states of maximum fissure-tubercle contact (maximum intercuspidation).
In such cases, using a permissive splint with an anterior median contact point can achieve relaxation of the active state of the muscles for 1-5 minutes. After some time, with the help of a splint it is possible to achieve complete deprogramming of the jaw.
- The occlusal surface covers only the central incisors with the formation of perpendicular contact with the antagonist central incisors. Chairside deprogramming can be done using Luciajig and modeling material.
- The patient should be informed of the need to move the jaw forward/backward along the occlusal surface, after which the position of the jaw is deprogrammed by retrusion over 1-2 minutes. As a rule, the mandible relaxes quite quickly if the articular head is already positioned in the fossa and the lateral pterygoid muscle is adequately relaxed.
- When performing the TMJ orthopedic stress test during the bimanual Dawson's maneuver, there should be no signs of tension or pain.
- Occlusal supercontacts in the central position are easily identified after removal of the deprogrammer.
Deprogramming is a diagnostic manipulation; it allows you to compare diagnostic models in the centric relation, and also helps to conduct a more in-depth analysis of the occlusion and determine the degree of correction required.
Occlusal-muscular parafunctions develop as a result of non-compliance with the criteria for static and dynamic occlusion. After all, problems arise not only with an incorrect bite, but also with excessive chewing loads, which develop the muscles that lift the lower jaw. The combination of incorrect occlusal relationships with parafunctional habits provokes even more disorders in the structure of the masticatory apparatus such as headaches, abrasion facets, muscle discomfort, etc.
Permissive tires with a front medial contact point are capable of:
- Correct malocclusion.
- Reduce the force of muscle activity by separating the distal teeth.
Correction of pain symptoms can also be carried out using similar splint designs, and pain, as a rule, disappears within 24 hours - 1-4 weeks. HTT splints are ideal for the treatment of occlusal-muscular parafunctions.
B-splints are made directly in the blade using 1.5 mm Biocryl (GreatLakes Orthodontics), BIOSTAR® (ScheuDental, Iserlohn, Germany), orthodontic composite and a press. Factory-made HTTs are coated with acrylic directly in the chair and thus customized (KellerLaboratories, Inc (Fenton, MO).
This approach is very effective in the initial phase of splint therapy. When symptoms disappear, an occlusal analysis and appropriate occlusal corrections are performed. In most cases, symptoms do not return even without further use of the splint.
On the other hand, parafunctional habits can pose a significant problem for the clinician even in the absence of obvious occlusal disorders. In some cases, symptoms of parafunction remain even when complete occlusal correction is achieved. When clenching, even under conditions of ideal occlusion, soreness of the temporal and masticatory muscles is observed. In order to avoid feelings of discomfort in the morning, the patient must use a splint at night. It is also important to consider changes in the pattern of parafunction throughout the day and the biological response of the dentition to splint, which can be recorded using a jaw movement analyzer (Bioresearch Associates, Milwaukee, WI). Patients with muscle pain typically keep their teeth in contact even in a “resting state.” This daytime muscle hyperreactivity provokes fatigue and even headaches. A night guard allows you to protect the dentofacial apparatus from nocturnal parafunction, and teeth from pathological abrasion. However, it must be remembered that the use of segmented structures can sometimes provoke intrusion of some teeth and super-eruption of others (which are not in contact with the splint). To prevent this effect, it is advisable to use a double splint on the upper and lower jaws (Fig. 13).
Rice. 13. Double B-slint covering all teeth with anterior midline contact point
Permissive full contact splints allow for a traditional approach to the treatment of occlusal-muscular problems. The use of these structures for 20 days already provides an effective rehabilitation result. Patients themselves note the disappearance of symptoms that previously worried them. A 20-year follow-up of treatment results showed that only 10% of patients after splint therapy required the use of muscle relaxants and sleeping pills. Correction of parafunction is carried out through the constant separation of the distal teeth, which, in turn, reduces muscle soreness, tense muscle pain, and migraines.
Joint lesions often manifest as partial or complete anterior disc displacement. Disc slippage is often associated with:
1) with macrotrauma;
2) with microtrauma, which can be caused by:
a) persistent excessive compression of the joint (parafunction);
b) anterior tension of the disc from sustained contraction of the superior convexity of the lateral pterygoid muscle (malocclusion, parafunction);
3) with a “weak link” in the system as a result of impaired collagen production, ligament weakness and hormonal imbalance.
Partial disc displacement usually develops on the lateral side of the condyle (Piper stage III) (Fig. 14).
Rice. 14. Lateral displacement of the disc with a normal head-to-disc relationship
Treatment using occlusal splints aims to achieve three main goals:
1) the formation of a harmonious interaction between the occlusion, muscles and joints;
2) reducing the load on damaged joint tissues;
3) elimination of symptoms associated with intracapsular edema, inflammation and muscle pain.
Full permissive splints (Fig. 15) are usually prescribed for several reasons:
It is believed that the contact of all teeth allows the load to be distributed over a larger area, thus reducing the load on the weakened joint. With proper distribution, only 5% of the load is transferred to the joint, the rest is “extinguished” by the teeth. The reduced load on the joint, in turn, allows for decompression of the retrodisc space and creates better conditions for healing of the affected area. In cases of partial disc displacement, the use of a permissive splint with an anterior midline contact point provides effective clinical results. In addition, these splint designs are also highly suitable for controlling parafunctional forces by dissociating the distal teeth. Some clinicians are concerned that a permissive splint with an anterior contact point may increase the risk of further disc displacement.
Rice. 15. Permissive splint with full contact on the lower jaw with contact of all teeth during joint positioning
To make a final decision when choosing a splint, additional studies of the joint reaction need to be conducted. We recommend using full permissive splint designs.
Other clinicians are concerned that a permissive splint at the anterior midpoint may pose a risk of further disc displacement. Let's consider these contraindications. Releasing the lateral pterygoid muscles reduces tension forces on the disc anteriorly. Due to the presence of hard and soft tissue damage, more time is required to achieve adaptive stability in the setting of partial disc displacement. Typically, the rehabilitation period takes from 6 to 8 weeks and is combined with the use of anti-inflammatory drugs.
Expected Result
It should be immediately noted that the final result of treatment is observed after 3-6 months. Although certain positive effects can be seen within 2-3 weeks (for example, reduction or complete disappearance of pain).
With high-quality manufacturing of the device and the patient following all the doctor’s recommendations, in most cases the following changes appear:
- Thanks to the presence of the splint, the muscle load of the dentition is distributed evenly.
- The functions of damaged joints are restored.
- Joint pain and headaches disappear.
- The bite is evened out.
- There is a gradual restoration of tooth enamel.
- The general condition of the oral cavity improves.
The final verdict on the effectiveness of treatment is made by the attending physician. If necessary, a repeat course should be taken after a break.
Conclusion
Complete disc displacement (Piper stages IV-V) is a complex disorder in the joint structure that may be amenable to splint therapy (Fig. 16). Patients with a displaced disc in both the lateral and medial directions are considered chronically unstable and are likely candidates for surgical intervention. Acute types of lesions most often involve compression and overload of the densely innervated and vascularized retrodiscal space, while chronic lesions involve the possibility of ligament perforation, scar tissue formation, and bone-to-bone contact with the development of osteoarthritis.
Rice. 16. Complete disc displacement with load on the retrodisc space
Splint therapy allows you to stabilize the joint and provide conditions for its proper functional adaptation and remodeling. In stages IV-V according to Piper, the duration of splint therapy can be up to 3 months, and in the future the treatment period can be extended based on individual conditions.
If the joint cannot be fully positioned without discomfort, a rigid wax register must be obtained with the patient tilted slightly forward. If, with such a register, the patient is able to bite without discomfort, diagnostic models can be cast on it, which are positioned using a face bow. Splint correction is carried out over several weeks until the joint has fully adapted and is in proper position. If the affected joint can be positioned without discomfort in a sufficiently anterior position, it is necessary to make an anterior repositioning guide splint. Manufacturing is carried out in a similar manner to the preliminary preparation of a wax bite register. In such cases, the patient needs up to 2 weeks before he can again use a complete permissive splint or before he is referred for surgical treatment due to the ineffectiveness of splint therapy.
Wearing rules and care
The effectiveness of treatment using the described method largely depends on compliance with certain rules for using the product. It is important to follow the recommendations received from your doctor during installation:
- The splint should be worn for periods specified by your doctor.
- If intermittent wearing is recommended, then during storage it should be kept in a closed container filled with a special solution.
- Before putting on the splint, be sure to brush your teeth and rinse the product itself in clean water.
- Be sure to visit your dentist regularly to have your device adjusted. The first visit is usually scheduled 2-3 weeks after installation. The timing of further visits is determined by the doctor.
Attention! After installing the occlusal splint, some time (the first few days) is required for adaptation. Sometimes diction may be impaired.
conclusions
It is essential that clinicians have a thorough understanding of all aspects of the dynamics of the masticatory system. Differential diagnosis by screening muscle function, joints and dental occlusion allows us to identify the main symptoms and signs of pathologies. Malocclusion and parafunction can be corrected through the use of splints described in this article. Joint pathologies can also be corrected using splints, however, given the etiology of their occurrence, this type of therapy is not always completely suitable for long-term stabilization of the TMJ.
Article published with permission from: AEGIS Communications
Translation: Miroslav Goncharuk-Khomin, Yulia Devyatko
Source: aegisdentalnetwork.com
Types of devices
During manufacturing, the splint is given a configuration that has a therapeutic effect, which depends on the specific clinical picture. Each occlusal splint is individual.
Depending on the functionality, the following types of splints are distinguished:
- Decompression. Designed to relieve muscle hypertonicity, normalize the occlusal load on the teeth, and prevent tooth abrasion. One of the most common pathologies treated with decompression splints is bruxism.
- Relaxation. Relaxes the chewing muscles.
- Positioning. The jaws and dentition are set in a normal occlusal position.
- Replicating . Corrects the position of the jaws relative to each other.
- Stabilizing. The lower jaw is returned to the correct position, in which the condyle moves to the center of the TMJ.
Which plates are most effective for straightening teeth in adults? Come here to find out when the use of the Brückl-Reichenbach apparatus is justified.
At this address https://dr-zubov.ru/ortodontiya/apparaty/trejnery/dlya-ustraneniya-problem-t4a.html we will talk about the use of T4a trainers for the correction of malocclusions in children.