The significant prevalence of dental caries in children determines the relevance of its prevention. Dental care for children should be preventive. Only under this condition does a real reduction in major dental diseases become possible [1, 2, 6].
Today, local fluoride prophylaxis is recognized as more effective than systemic fluoride prophylaxis [9]. In this case, the factor of the constant presence of fluorides on the tooth surface is important [8, 10].
According to WHO, fluoride-containing toothpastes occupy approximately 95% of the European toothpaste market, which, when used regularly, reduce the increase in caries by 25% [7].
Under natural conditions, the source for the entry of the main structural elements of calcium and phosphorus into the enamel is the oral fluid. However, the remineralizing potential of saliva allows stopping caries at the spot stage only in 50% of cases [6]. Therefore, to increase the caries resistance of enamel, it is necessary to use products that include components that increase its mineral saturation.
Evidence has appeared in the literature that the remineralization process is supported enzymatically; in particular, the inclusion of phosphates and calcium in tooth enamel under the influence of phosphatases is significantly activated. The activity of these enzymes increases in the presence of chlorine and magnesium ions. The substrate for alkaline and acid phosphatases is calcium glycerophosphate. Studies using immobilized alkaline phosphatase have demonstrated that it is in the presence of glycerophosphate that the mineralization process of teeth is most successful. The reason for this may be a greater acceleration of the formation of apatite under the action of immobilized alkaline phosphatase than brushite or whitlockite [5]. In addition, to carry out the processes of mineralization and remineralization, the presence of biopolymers and hyaluronic acid in the interprismatic spaces of the enamel is necessary [3].
The purpose of the study was to increase the caries resistance of dental enamel in children and adolescents by using a complex remineralizing fluoride-containing coating with tricalcium phosphate.
What is caries resistance?
In dentistry, a condition called caries resistance is often encountered, but what does this mean? How is this condition characterized?
Attention! Caries resistance is considered to be increased resistance to carious lesions. Increased resistance to caries is usually observed in people who adhere to a healthy lifestyle. In addition, this condition is observed in people who are not burdened with any pathologies or severe complications and who follow a balanced diet. Tooth decay resistance properties are achieved by consuming essential vitamins and minerals to strengthen tooth tissue and bones.
Caries is a disease of our time; it occurs in almost every person in one form or another. But there are those who have innate immunity, this phenomenon is called caries resistance.
Relevance
. Currently known methods of preventing dental caries can effectively combat this disease. However, in order to select the most effective means of caries prevention, it is necessary first of all to clarify the schemes and indications for their use. This is closely related to the possibility of dynamically determining the individual resistance of dental hard tissues to caries, depending on the state of the body and treatment and preventive measures.
Purpose of the study
— to compare the effectiveness of existing methods for assessing caries resistance to improve control of enamel condition and the possibility of early diagnosis of caries and determining the effectiveness of prevention methods.
Material and methods.
The study included 40 patients aged 32 to 45 years, with an average age of 35 years. Patients were divided into 2 groups, randomized by gender, age and level of caries resistance. All patients underwent a clinical examination of the mouth with determination of the OHI-S index. To assess the condition of the enamel, the level of caries resistance was determined using the V.B. method. Nedoseko (V.B. Nedoseko, 1988) and performed an acid biopsy (V.K. Leontyev, V.A. Distel, 1975 modified by M.Yu. Zhitkova, 2000) with the calculation of the calcium-phosphorus ratio (Ca/P coefficient) , as well as the KOSRE test (V.K. Leontyev, T.L. Redinova, G.D. Ovrutsky, 1988), reflecting the rate of enamel mineralization. Patients in both groups received instruction in oral hygiene, dental treatment according to indications, and professional hygiene. Those observed in the main group were additionally prescribed the remineralizing gel Tus Mousse, which they rubbed into the enamel of their teeth 2 times a day, morning and evening, for 30 days. After 1 month, an acid biopsy was repeated in both groups to assess the condition of the enamel. To determine the correspondence between the two methods, assessing caries resistance (V.B. Nedoseko method, acid biopsy method), a correlation analysis of the obtained indicators was carried out.
Results.
The level of resistance in each group was not higher than moderate, the level of intensity of caries KPU was 15, the initial value of the Ca/P coefficient was 0.29.
The correlation coefficient between the level of caries resistance and the Ca/P ratio was quite high and amounted to 0.72. Recovery of the focus of demineralization after acid biopsy in the control group occurred after 25±5 days, in the main group - after 10±2 days ( p
<0.01), indicating a higher rate of remineralization with the drug used.
By the end of the month of observation, the Ca/P coefficient increased in the control group to 0.32, and in the main group against the background of the use of Tus Mouss gel - to 0.39 ( p
= 0.19 and
p
= 0.03 relative to the initial level, respectively). The Ca/P coefficient in the main group after remineralizing therapy was less correlated with the level of caries resistance. In the control group, the correlation coefficient was 0.63, in the main group - 0.32. This is explained by the fact that in the control group after a month the level of mineralization (according to V.B. Nedoseko) differed little from the initial one. In the main one, enamel resistance increased by 22% compared to the primary data.
Conclusion.
The acid biopsy method allows you to record changes in the condition of the enamel in a shorter time. Determination of the level of caries resistance using the V.B. method. Insufficient and indicators of acid biopsy of enamel are comparable, however, enamel biopsy allows not only to predict the development of caries, but also to quickly monitor the dynamics of caries resistance, which is necessary for studying different schemes and methods of prevention, choosing the most effective and economical, depending on the individual characteristics of patients.
Features of caries resistance
Caries resistance includes several main properties of enamel:
- Degree of acid resistance;
- Microhardness;
- Permeability.
The development of caries depends on the following factors:
- On the degree of aggressiveness of various factors;
- From the condition of the enamel.
It follows from this that during the pathogenesis of the development of dental caries, the main role is played by the decalcifying effect of organic acids of microbial origin. It is believed that the degree of resistance of the enamel structure to acid demineralization directly reflects all the properties of resistance to carious lesions.
Caries resistance – resistance of dental tissues to carious effects. Caries resistance includes not only the condition of the tooth tissues, but also the condition of the oral cavity, oral fluid, and the condition of the body as a whole.
Therefore, resistance to dissolution is considered the most important quality of enamel, which allows maintaining the integrity of the structural and functional appearance in the presence of acid-forming bacteria inside the oral cavity and plaque. As a result of numerous studies, it was revealed that the degree of solubility of enamel tissue on different surfaces differs. The gingival areas of all teeth have the highest degree of solubility. This is due to the fact that it is in these places that there is a reduced level of mineralization. According to V.K. Leontiev, which was put forward in 1977, various factors may underlie the heterogeneous structure of enamel:
- Differences in mineralization of different parts of the tooth;
- The presence of various defects in the structure of the crystalline lattice;
- Individual qualities of interactions between the protein matrix and the mineral phase and other reasons.
Professor Okushko V.R. in 1984 determined that the acid resistance of enamel is associated with the properties of centrifugal permeability, due to which cerebrospinal fluid is released on the surface of the enamel. As a result of a series of experiments, it was found that by regulating the speed of movement of the cerebrospinal fluid, it is possible to change the acid resistance, and therefore the resistance of teeth to caries. In general, acid resistance and caries resistance depend on the properties of dental tissue and enamel. These factors are provided by the functional and structural features of the tooth structure.
Material and methods
To achieve the stated goal of the study at the Department of Pediatric Dentistry with Orthodontics at VSMU named after. N.N. Burdenko, as well as on the basis of the state educational institution of the Voronezh region “Boarding School No. 1 for orphans and children left without parental care,” a prospective cohort examination of the oral cavity of 138 children was conducted, of which 27 (19.6%) were aged 7-10 years old, 39 (28.3%) children aged 10 to 14 years and 72 (52.2%) adolescents aged 14-16 years old, living in the same type of environmental conditions of Voronezh, receiving the same nutrition, having intact dental row, foci of initial demineralization of enamel, as well as carious cavities of teeth.
In accordance with the purpose of assessing the effect of a fluoride-containing coating with tricalcium phosphate, a study was carried out on 45 patients with high caries resistance, without carious cavities and foci of initial demineralization of teeth, covered with a small amount of soft plaque, who made up the 1st group, 62 patients with sufficient average caries resistance, having foci of initial demineralization and primary foci of destruction of enamel and cement, as well as carious lesions of only chewing teeth, the absence of pulpless teeth, the presence of a small amount of soft plaque, according to the surveyed - new carious cavities did not appear every year - group 2 and 31 patients with reduced average caries resistance, having carious cavities in the chewing frontal teeth, the presence of several cavities in one tooth, the presence of pulpless teeth, a significant amount of plaque on the teeth, according to the surveyed, the annual appearance of new carious cavities, the rapid “loss out” of fillings within 1-2 years — 3rd group [4].
All groups were divided into 2 subgroups to evaluate the effectiveness of treatment with the use of therapeutic and prophylactic fluoride-containing coating with tricalcium phosphate and without the use of this product, but using individual oral hygiene products.
In laboratory conditions, 10 extracted teeth of patients aged 7 to 16 years were examined for orthodontic indications. Intact teeth were subjected to special research methods: scanning electron microscopy, X-ray spectral microchemical and energy dispersive analysis.
The objectification of clinical data was facilitated by the use of laboratory research methods, the results of which were recorded at certain time points - a clinical examination after 6 months. When carrying out the study, ethical principles were observed, written consent was obtained from the administration of boarding school No. 1, as well as the Department of Education, Science and Youth Policy of the Voronezh Region for the examination and implementation of preventive measures.
Dental fluoride material Clinpro White Vamish is a complex remineralizing fluoride coating with tricalcium phosphate, containing fluoride in the form of 5% sodium fluoride and the innovative ingredient tricalcium phosphate with fumaric acid, which does not allow it to react with the fluoride inside the package until the product is applied on the teeth. The coating is an alcohol solution of a modified resin. Clinpro White Vamish is sweetened with xylitol and has a pleasant minty flavor. The product is supplied in packs containing a single dose of 0.5 ml. Each 0.5 ml dose contains 25 mg of sodium fluoride, which is equivalent to 11.3 mg of fluoride ion (22,600 ppm fluoride).
Visible and accessible tooth surfaces were assessed by visual inspection in good light using a dental mirror and probe, and vital staining of the teeth with a 2% aqueous solution of methylene blue. To assess the hygienic state of the oral cavity, the expanded hygienic index according to Fedorov-Volodkina was determined; the plaque index was assessed using a probe from four surfaces without staining with preliminary drying with an air jet.
To assess the rate of reduction in caries growth, we proposed an index of clinical and laboratory assessment of the resistance of hard tissues of teeth (ICLORZ) as a more sensitive assessment result to initial changes in enamel, determined in combination with X-ray diagnostics, electrometric diagnostics and light-induced fluorescence, in contrast to the CPZ index (Table 14].
Table 1. A set of methods for clinical assessment of the condition of hard dental tissues Note. * — R0 — no signs of destruction; R1 - demineralization of the outer half of the enamel in the affected area; R2 - demineralization of the entire enamel layer in the affected area; R3 - demineralization of enamel and the outer half of dentin in the affected area; R4 - demineralization of enamel and deep layers of dentin in the affected area.
If you have filled teeth, the score is given depending on the electrometric resistance at the border of the filling and the hard tissues of the tooth.
The index was calculated as the ratio of the sum of points obtained to the total number of examined teeth in the oral cavity.
Intraoral X-ray diagnostics were carried out using a dental apparatus de Götzen srl (Italy) sistema radiografico per diagnosi intraorale - x-ray system, electrometric diagnostics of hard dental tissues were carried out using a DentEst apparatus, Russia. The measurements were carried out at a constant voltage of 4.26 V, and the results obtained in microamperes were recalculated to the resistance value of the hard dental tissues under study, taking into account the factor of the full maturation of the enamel. The assessment of light-induced fluorescence of hard dental tissues was carried out using an LED activator LED active 05, Russia, at a wavelength of 530 nm, illumination of 100,000 lux, and also a wavelength of 625 nm at a radiation power density of 140 mW/cm².
To determine the microcrystallization index of oral fluid on a drop of this liquid, the ratio of the number of ocular grid points projected on the crystals to the total number of ocular grid points projected throughout the entire drop of oral fluid was calculated.
The buffer capacity of saliva was determined using the CRT buffer kit, and the acidity of the oral fluid was determined using the I-500 basic ion meter.
Scanning electron microscopy and X-ray spectral microchemical analysis (XMA) of 10 extracted teeth were assessed using a low-vacuum scanning electron microscope model JEOL JSM-6380LV (Japan). The distribution of chemical elements in the area of the interface of the fluorine-containing coating and tricalcium phosphate with tooth tissues was studied by micro-X-ray spectral mapping of transverse chips of teeth using an INCA-250 energy dispersive analysis (EDA) system. The planar distribution of chemical elements was assessed by coloring the X-ray image with different colors specified by the operator.
Statistical analysis of the materials obtained as a result of the study was carried out using the mathematical software package Statistica 6. X, Biostat, which is an integrated environment for statistical analysis and data processing.
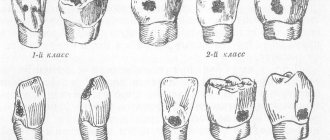
Caries of enamel, dentin, cement
In dentistry, there are several classifications of caries depending on the affected area, the degree of disease activity and the depth of the lesion. The classification of the World Health Organization (WHO) is considered the generally accepted and most popular. According to it, the disease is divided into:
- enamel caries - superficial caries of dental tissue;
- Dentin caries - damage to the tooth tissue under the enamel;
- Cement caries is a root lesion that occurs after exposure of the tooth root.
If caries on tooth enamel can be stopped using non-invasive or minimally invasive methods, then it will no longer be possible to cure later stages without surgical intervention.
The effectiveness of non-invasive treatment methods
If the damage caused to the tooth is insignificant, and the enamel is sufficiently dense, treatment of enamel caries in the white spot stage can be carried out without preparation and filling. In this case, the affected area is ground and polished, which avoids the recurrence of the disease. After this, the tooth is locally fluoridated, and the process of restoring the enamel from the inside begins. This treatment method is called remineralization. Fluoridation can also be done at home - using special preparations - but only after consulting a doctor.
Also, modern methods of non-invasive treatment of enamel caries include: chemical-mechanical treatment (infiltration), air-abrasive treatment and ozone treatment. All these methods allow you to do without a drill and carry out treatment with virtually no discomfort for the patient. At the same time, it is possible to preserve healthy tooth tissue to the maximum - the microhardness of the enamel is damaged during enamel caries, and all of the above methods allow you to act only on softened tissue, without affecting the healthy parts of the tooth.
Regardless of the chosen technique, in order for the treatment of dental caries to be effective and the disease not to recur, the participation of the patient himself is important. Only a conscientious approach to hygiene will help maintain oral health.
Treatment of enamel caries
Treatment of enamel caries can be carried out using several methods: both with and without preparation. General list of measures for the treatment of enamel caries:
- oral hygiene using fluoride toothpaste
- remineralization
- sealing
- taking special medications to strengthen teeth
- tooth preparation and filling.
The last point applies when a pronounced roughness or small cavity has formed on the enamel: in this situation there is no other way to do it.
Invasive methods for treating dental caries
- Conventional filling: in this case, the preparation takes place quite quickly and without anesthesia; the resulting cavity is processed and filled with a composite material.
- Filling hard-to-reach places: carried out if it is impossible to gain access to the affected tissue in any other way (for example, between teeth). To do this, a small part of the healthy tissue must be removed, only after this the specialist will be able to proceed directly to removing the carious lesion and filling the resulting cavity.
In some cases, a specialist may suggest sealing fissures - natural grooves on the teeth - to prevent the accumulation of food debris and reduce the likelihood of the development of carious bacteria. This is a fairly effective way to prevent the disease.
Clinic and diagnosis of enamel caries
The difficulty in diagnosing initial enamel caries in the spot stage is that the patient does not experience any discomfort - the tooth reacts normally to changes in temperature, sweet, sour and salty foods and only in rare cases, for example, if enamel caries develops in the area of the sensitive neck of the tooth, mild discomfort is possible. Visually, enamel caries can appear as a white spot or a small cavity. The tooth surface in the affected area may become slightly rough.
One of the most insidious clinical cases of enamel caries is lesions in the interdental spaces. Since this area is hidden from view, pathology can often only be detected at a later stage.
What complicates the diagnosis of enamel caries is that damage to tooth enamel is not always caries. Fluorosis, erosion, abrasion of enamel and hypoplasia have similar symptoms. For example, both fluorosis and hypoplasia are accompanied by white spots or roughness on the enamel.
Types of diagnostics
- Visual examination
in the clinic using drying - this allows you to detect a rough surface on smooth enamel. - Diagnosis
of caries on tooth enamel using dyes: a quick and easy way to determine whether a patient is developing caries - or if it is just pigmentation. The fact is that with initial caries, tissue softening occurs in the enamel, and if the lesion is carious in nature, the dye will easily penetrate into the affected tissue and color it. With fluorosis or hypoplasia, staining will not occur. - Fluorescent diagnostics:
exposure of teeth to special ultraviolet lamps, during which healthy tissue begins to glow with a bluish or greenish light, but in the area affected by carious bacteria there is no similar effect. The method is quite accurate, but expensive.