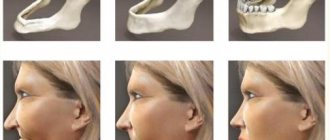
Unfavorable anatomical conditions include the low location of the bottom of the maxillary sinus in the upper jaw and insufficient distance from the alveolar crest to the mandibular canal. Often this reduction in bone height occurs due to tooth extraction. The removal of even one tooth entails changes in the entire dentition, chewing function is disrupted, as a result of which bone tissue atrophies.
Before implantation, it is necessary to carry out a set of measures aimed at the formation of bone tissue and giving the necessary volume of bone in the area of the defect. Bone volume can be restored using guided bone regeneration. Some surgeries to restore bone volume are also performed using guided regeneration techniques.
Why is the operation performed?
In the presence of a narrow ridge, it is impossible to carry out high-quality dental restoration, especially on toothless jaws. The jaw may have this shape naturally or acquire it as a result of atrophy, injury, removal of a tumor, or a previous disease. Indications for surgical intervention:
- Insufficient tissue volume.
- Thin alveolar process.
- Atrophy or other defects of the jaw.
Features of natural bone material
Transplants created from organic materials have their advantages and disadvantages. Depending on the type of osteoplastic substance, its abilities will differ. Each graft has two main properties:
- promotes the regeneration of the patient’s own alveolar tissue;
- is a supporting structure for bone cells and foundations for their restoration.
Natural materials of human origin are maximally capable of increasing regeneration. This effect is especially enhanced if, during the process of bone grafting, the patient is given, in addition to the graft, concentrated blood, previously taken from a vein and subjected to centrifugation. Synthetic structures are more aimed at providing support for the atrophied alveolar ridge.
Patients are often wary of getting transplants from animals or other people because of the risk of developing diseases or the perceived high likelihood of rejection. In fact, the process of creating osteoplastic material in dentistry undergoes a number of control checks before it is allowed into dental clinics. None of the grafts pose any threat to the patient, so the risk of infection can be eliminated. However, less successful engraftment is indeed typical for such structures, so the doctor must take into account the individual characteristics of a person’s health. For example, elderly people rarely receive autogenous grafts, since it is dangerous for them to perform the additional step of tissue collection.
Contraindications
The alveolar ridge splitting procedure cannot be performed if there is a risk of graft or implant rejection. This situation occurs in the body in the presence of serious pathological conditions, systemic diseases that can cause complications during or after surgery. Contraindications include:
- Allergic reaction to the materials used or anesthetics.
- The alveolar process is less than 2 mm in width and less than 10 mm in height.
- Diseases that reduce immunity (AIDS).
- Acute inflammatory processes in the oral cavity or body.
- Stomatitis, tonsillitis, sore throat, rhinitis.
- Metabolic disorders, including in bone tissue (osteoporosis, resorption).
- Incoagulability of blood.
- Acute viral, bacterial or fungal infections.
- Pregnancy and lactation.
- A course of radiation therapy (for oncology).
Guided bone regeneration
This method consists of carrying out measures aimed at creating conditions for the formation of bone tissue in the area of the defect. To do this you need:
- atraumatic surgical intervention;
- complete removal of fibrous tissue;
- filling the defect with biological material (bone graft, bone chips, hydroxyapatite, etc.);
- isolation of a defect filled with material using barrier membranes;
- suturing the wound.
Surgical technique
Treatment consists of the following stages:
- Preparation.
- Anesthesia.
- Section of the gums and periosteum.
- Delamination of soft tissues.
- Splitting of the alveolar ridge of the lower or upper jaw.
- Separating the edges of the bone.
- Introduction of the graft.
- Filling the free space with bone material.
- Installation of a protective membrane.
- Applying sutures to the gum.
- Recommendations for the patient.
Stages of surgery
The procedure for splitting the alveolar process includes the following stages: preparation, anesthesia and the operation itself.
The surgeon dissects the gum and bone tissue, after which one of two possible techniques is selected:
- installation of implants, filling the remaining space with osteoplastic material and membrane, after which sutures are applied;
- filling the cavity with bone material and performing implantation after engraftment several months later.
Recovery period
Recommendations for the patient:
- Eat soft foods.
- Carefully monitor oral hygiene.
- Apply antiseptic rinses to the suture area.
- Rinse your mouth after eating.
- Avoid physical activity and bad habits.
The postoperative period is the final stage of treatment, during which the mucous membrane heals and the graft engrafts. Patients are advised not to load the jaw and take care of the oral cavity. 4-5 months after the operation, implants can be installed and prosthetics can be performed.
As a result of reconstructive surgery, the oral cavity will be restored and ready for orthopedic treatment.
To the list of posts
Application of piezosurgical technique
A promising and proven piezosurgical technique is successfully used in complex clinical cases, such as critically small alveolar bones. The main advantages of the technique include efficiency, safety and accuracy.
The use of the piezosurgical technique when performing splitting of the alveolar process occurs with the simultaneous installation of two-stage implants.
The surgical intervention takes place under local anesthesia. The dental surgeon makes an incision in the mucous membrane in the projection of the apex of the alveolar process, separates the soft tissue, exposing the critically atrophied alveolar process. Using a piezo instrument, the dental surgeon splits the alveolar process longitudinally along the apex. After which the implants are installed, the remaining space is filled with osteoplastic material. The operation is completed by checking the primary stabilization of the implant, closing the wound with a mucoperiosteal flap and applying sutures.
Creation of special implants
Dental implantation in cases of bone tissue deficiency is possible only with the use of special implants that will be completely safe for the patient and will not allow the crowns to lose their natural appearance. For these purposes, special designs have been created that have the following features:
- Cone-shaped (allows easy entry into bone tissue);
- Cylindrical thread shape (exists in order to firmly fix the implant in the bone and minimize the risk of loosening and loss);
- Large spaces between the protrusions of the spiral in the thread (bone tissue quickly fills them, finally securing the implant);
- The length of the artificial root does not exceed 6 mm (the design elements made it possible to reduce its size as much as possible).
These implants have another distinctive feature, due to which they are used exclusively in operations without bone grafting: the structures do not provoke atrophic processes in bone tissue and do not lead to an increase in its deficiency. Over time, the artificial root will not become exposed and will not fall out. If you place an implant created without taking these features into account, the situation with a lack of bone tissue will only worsen.
How many lost teeth can be restored this way?
The technique makes it possible to restore any number of lost teeth. Even when implanting one tooth, the technology allows an incision to be made in such a way as to insert the implant into the bone without damaging the adjacent teeth. But most often, a narrow bone occurs in the absence of a large number of teeth, so specialists usually install two to four implants on each side.
Make an appointment
right now!
Snitkovsky Arkady Alexandrovich
Therapist, Orthopedist
Indications for bone splitting surgery
- Narrow ridge of the jaw, this often happens on the lower jaw;
- Long absence of a tooth in the jaw - during this time the bone decreases and it becomes insufficient for installing an implant;
- Anatomical features in which a person initially has little bone tissue.
There are implantation methods when bone grafting is not required, but they are not classical and should be considered individually with the dentist.
In order for the splitting of the bone crest during implantation to proceed as it should, two basic conditions must be met:
- Its minimum height should be 8 millimeters;
- The width of the bone should be at least 3 millimeters at its narrowest point.
Bone augmentation during dental implantation: indications
If there is a lack of bone material, it will not be possible to properly fix the implant in the jaw, which can lead to complications such as:
- loosening of the implant or its loss;
- perforation of the maxillary sinus;
- the occurrence of cracks in the tissues of the jaw due to a lack of bone width.
Based on CT images of the jaws, an experienced implantologist will be able to not only select the desired model of implants, but also determine whether the patient needs osteoplasty.
How bone grafting is done at St. Petersburg dentistry “GrandMed”
For reliable fixation of the implant, a sufficient amount of bone tissue is required, the deficiency of which can be compensated for by bone grafting. The surgical technique is chosen by the implant surgeon based on the structure and condition of the patient’s jaw bones. In our clinic, an orthopantomograph is used to identify problems with bone tissue - defects are easily detected by analyzing a panoramic image of the dentofacial system. If the situation is not so obvious, the patient is offered a computed tomography scan. A mandatory stage of preparation is the sanitation of the oral cavity, that is, the treatment of caries and its complications. Before the operation, it is necessary to do a general blood test and consult an ENT doctor.
Operation stages:
- Pain relief . For comfortable bone grafting, local anesthesia is sufficient - the patient is given an injection, and after a few minutes he is ready for surgery.
- Disinfection. The surgical area is carefully treated with special compounds that destroy surface pathogenic microflora to prevent them from penetrating deep into the tissue.
- Osteoplasty. The surgeon's procedure may vary; the main techniques include incision of the mucosa and detachment of the flap, formation of a cavity, placement of an inert preparation and application of a membrane.
- Completing the operation. The edges of the wound are sutured, the surface is disinfected and covered with a swab, which is removed after 20 minutes.
Patient reviews
In general, on the Internet on forums, patients speak positively about this operation, especially if it is performed on the upper jaw. After it, recovery is faster, especially when compared with grafting a bone block. A problem such as shifting of the installed bone material is much less common, that is, complications arise less often. Swelling and pain also go away very quickly. Patients are especially pleased that implants can be placed immediately during surgery, and not some time after bone grafting.
Possible complications of sinus lift
The risk of complications when performing various types of interventions always exists, so it cannot be ignored. This does not mean that a “bad” dentist was chosen or that the material for sinus lifting of the jaw was selected incorrectly. Even in conditions close to ideal, there remains the possibility of a small risk of complications.
After the intervention, elevated temperature, swelling, and pain in the jaw area are considered completely normal reactions of the patient’s body. All of them should disappear at the end of the third day. Bleeding and facial numbness disappear within 3-5 hours after sinus lift surgery. However, the hematoma persists for up to seven days, even after the procedure is successfully completed. If the above deadlines are not met, it is important to consult a doctor. Dehiscence of sutures, purulent runny nose, prolonged numbness of the face, repeated rise in temperature - all these are deviations from the norm that require an immediate visit to the doctor.
Most often, bone deficiency is observed on the vestibular side of the alveolar process. Many authors have proposed their own classifications of alveolar ridge defects, including Allen et al, Seibert, Cawood and Howell, Studer, and others.
In accordance with the classification of Wang and Shammeri, defects of the alveolar process are distinguished by height, thickness and combined. Splitting of the alveolar process is recommended for thickness and combined defects.
It is generally accepted that bone augmentation techniques are less predictable and cause a higher percentage of complications than isolated implant treatment.
Today, methods for reconstructing the alveolar process are available using:
titanium mesh or foil;
· resorbable or non-resorbable membranes;
· titanium modules or screws for osteosynthesis;
· bone materials (autogenous, allogeneic, xenogeneic blocks);
· 3D-techniques; splitting of the alveolar process and their combinations.
The success rate of different techniques varies. For example, the effectiveness of GBR varies between 85 - 98%, while the newly formed bone tissue, from the point of view of implantation, turns out to be as close as possible to natural bone.
However, this technique requires much more time. One of its complications is membrane exposure, which can cause loss of the implant and bone in the intervention area.
Autotransplantation of bone blocks in the form of inlays or onlays, according to various sources, ranges from 60% to 93%. However, all publications note a high risk of resorption of autogenous bone grafts and a long healing period.
Technique using bone materials for splitting the alveolar process
It is known that it is more difficult to achieve success in restoring the alveolar process after vertical atrophy than horizontal atrophy. To eliminate the consequences of horizontal atrophy, you can use the technique of splitting the alveolar process.
The classic surgical protocol is as follows:
· Incision of the mucosa, submucosa and periosteum behind the grafting line; making releasing incisions.
· Peeling of the mucoperiosteal flap.
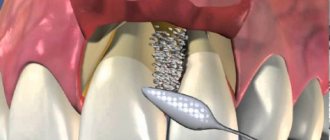
· Performing bone cuts along the apex of the alveolar process and vestibular surface within the compact lamina.
· Expansion of the bone using any of the available methods.
· Introduction of bone material.
· Stitching.
This technique was proposed in the early 90s of the last century. Despite the wide possibilities of clinical application, the intervention has a number of disadvantages:
· Narrow range of conditions for carrying out.
· Possibility of longitudinal jaw fracture.
· Excellent manual skills required.
· Greater discomfort experienced by the patient during the operation.
· Limited volume of augmentation replanting.
· Limitation of use within individual dentition defects.
Of course, to perform splitting of the alveolar process, certain conditions must be met, otherwise this technique cannot be successfully implemented.
Conditions for splitting the alveolar process:
· The width of the top of the ridge should be about 3 - 6 mm.
· The alveolar ridge is narrow in the coronal part and wide in the apical part.
· The alveolar process must have a spongy part.
· Possibility of fixing at least 1/3 of the implant apical to the splitting zone.
· Possibility of installing an implant of sufficient length.
· Possibility of covering with soft tissues.
Many modifications of the alveolar process splitting technique have been proposed. In 1994, Summers proposed a technique for splitting the alveolar process with osteotomes.
Many surgeons use a combined flap (incomplete-complete-incomplete) to split the alveolar process. That is, the periosteum is peeled off only in the area of the future cut. This makes it possible to maintain trophism, flexibility and elasticity of bone tissue, as well as prevent excessive resorption and traumatic fracture.
When constructing the flap, Dehasjuk et al do not recommend releasing incisions.
Here are several methods for expanding the alveolar ridge:
· Expansion with osteotomes (as a rule, pointed conical osteotomes are used according to the Summers method).
· Expansion with an implant (special implants are used for this, which are used only for the splitting technique).
· Expansion with osteotomes and an implant, or a combined technique (the so-called expansion with closed sinus lift).
The technique discussed below will use expansion of the alveolar bone using a chisel. This technique makes it possible to easily, without special manual skills, expand the alveolar process. Its disadvantage is the significant discomfort experienced by the patient during the operation.
A free gingival or connective tissue graft can be used to provide adequate soft tissue coverage.
Some authors believe that transplantation of a graft before osteoplastic interventions is inappropriate, since after augmentation the number of attached keratinized gums will significantly decrease and transplantation will not make sense. In addition, a break of at least 3 months is needed after soft tissue transplantation for maturation before osteoplastic measures.
On the other hand, soft tissue grafting is appropriate when soft tissue augmentation is necessary to adequately cover the augmented area.
Another argument in favor of autotransplantation of soft tissues in the area of clefting of the alveolar process is the need to convert a thin periodontal biotype into a thick one to form an aesthetic contour and imitate gingival papillae at the second stage.
So, let's consider each stage of treatment and the role of bone materials in the splitting of the alveolar process in combination with transplantation of free flaps.
First surgical stage
In the edentulous area within the attached keratinized gum, an incision is made with an offset towards the tongue in the lower jaw and the palate in the upper jaw. In this case, the incision in the lower jaw is shifted so that approximately 2 mm of keratinized gum remains on the tongue side.
On the upper jaw, the incision is shifted towards the palate, according to anatomical conditions. On the vestibular side, instead of releasing incisions, incisions are made around the necks of natural teeth. As a rule, the vestibule of the oral cavity deepens in the area of intervention.
To preserve the blood supply to the vestibular cortical plate, the bony crest is preferably left covered by periosteum. To separate the vestibular and lingual parts of the alveolar process, the cut is carried out with a surgical bur. Splitting is performed with straight or angled tips.
The limit to the degree of separation of the bone plates is the elasticity of the bone crest and the diameter of the implant that is planned to be installed.
After expansion is completed, the bed is prepared for implants using cutters with diameters that are selected in accordance with the manufacturer’s protocol.
Implants are installed manually. Bone material in the form of a gel is injected into the splitting site. The insufficient amount of soft tissue in the upper jaw can be compensated with local tissues (apical displacement of the flap), in the lower jaw - with free gingival or connective tissue flaps.
The proposed protocol provides for a two-stage installation of implants. If premature spontaneous opening of the implant occurs, a gum former is installed, the height of which depends on the formed volume of soft tissue.
The sutures are applied with silk and polyamide, and the graft itself is fixed with materials based on polyglycolic acid.
Examination of the patient and removal of sutures are planned 5-7 days after surgery. In the postoperative period, patients can optionally have permanent adhesive structures made.
Second surgical stage
To control integration before the second stage, the following indicators are assessed:
· Patient complaints.
· X-ray data.
· Stability of the implant at the time of deployment, etc.
The second surgical stage is recommended to begin at the following times: on the lower jaw after 10 weeks, on the upper jaw - after 14 weeks. As a rule, during healing in all cases it is possible to achieve an increase in the width of the alveolar process and the amount of attached keratinized gum.
Exposure is carried out using various methods, depending on the clinical situation and the need to form an aesthetic contour or imitate gingival papillae.
Orthopedic stage of treatment
In accordance with the described method, the orthopedic stage begins 23 weeks after opening the implants. For prosthetics, you can use both individual zirconium oxide abutments and factory-made abutments.
The choice of abutments is determined by the characteristics of the orthopedic design (metal-ceramic or all-ceramic), the height of the smile and aesthetic requirements, as well as the wishes of the patient.
Conclusions and recommendations
According to Dehasjuk and a number of other authors, this augmentation technique and the use of bone materials for splitting the alveolar process have many advantages.
Firstly, this technique is less traumatic compared to others used for lateral augmentation. The easy postoperative period and the absence of an additional surgical area for autologous bone collection make it possible to widely use this technique.
Secondly, there is the possibility of combining the technique with the installation of dental implants in one stage. Its use almost always provides high levels of primary stability and allows the use of an early loading protocol.
Thirdly, due to the absence of the need for the use of additional means, the cost of the operation is significantly reduced and, as a rule, surgery is not required to remove membranes, meshes, screws and the like.
The fourth advantage is the fact that bone grafting is carried out into a three-walled (according to some classifications, four-walled) defect with a high osteogenic potential. This promotes rapid replacement of the material with bone tissue.
The healing period when using the above-described treatment method is much shorter than with other reconstructive methods, and is about 2-4 months.
By splitting the alveolar process, the vestibular fragment is significantly displaced, thereby partially or completely compensating for the unaesthetic contour that is formed due to bone resorption.
Loss of an implant when using this technique is considered a fairly rare occurrence, which is usually observed in the reparative phase. And even after disintegration, the resulting volume of bone tissue remains to a large extent.