If surgical dentistry used to be primarily concerned with the removal of teeth, now its main tasks are their treatment and preservation. Even if the situation seems completely hopeless, competent doctors will try to cope with it. Also, the tasks of surgery include the treatment of some other inflammatory processes in the oral cavity, removal of tumors, abscesses, and various congenital and acquired defects.
But, in addition to these tasks, surgery also performs the following:
- Study of oral diseases;
- Diagnostics and development of new diagnostic techniques;
- Development and implementation of new surgical treatment methods;
- Dental implantation;
- Surgical relief from problems with the facial and jaw bones, oral organs and neck.
Why is wisdom tooth germ removal necessary?
Progressive specialists are confident that removing the wisdom tooth germ is truly the right decision.
Some Russian dentists, who continue to use outdated methods in their work, are trying to treat wisdom teeth. As a rule, this subsequently causes great harm to the patient. According to specialists from dental clinics in the USA, Israel and European countries, in such a situation only the removal procedure will help solve the problem.
Western experts have every reason for such confidence. According to the results of long-term studies that covered a significant part of the population, in 99% of cases, retained wisdom teeth resulted in serious complications for patients.
If you delete, then all four?
Yes, two wisdom teeth on the top and two on the bottom jaw. If you only extract at the bottom, the upper teeth may move downwards because they have lost the neighbor they were in contact with. And curvature of the dentition will occur. Which will entail a click in the joint (TMJ) and further complications.
Removing an upper wisdom tooth is usually easier than removing a lower one because the upper jaw has less dense bone tissue. In addition, the lower eights often have more branched roots, which somewhat complicate the operation and increase the recovery period. An X-ray or computed tomography scan is required before the wisdom tooth removal procedure!
The main signs of these complications were:
- discomfort caused by biting the cheek, which leads to the appearance of bedsores and ulcers, due to which cancer of the oral cavity develops;
- pressure on the dentition, contributing to its curvature and the development of aesthetic defects;
- additional load and compression of the front teeth, gradually affected by periodontitis and periodontal disease;
- rapid destruction, problems with removing damaged teeth, injury to bone and gum tissue;
- the development of purulent-inflammatory processes in the throat and middle ear, the elimination of which requires complex surgical intervention;
- Difficulties with hygienic care, in the absence of which an unpleasant odor appears, teeth rot and inflammation of soft tissues occurs.
These undesirable manifestations once again confirm that every patient requires removal of the wisdom tooth germ. It should be noted that this complex dental procedure can only be entrusted to a highly qualified specialist. Confirmation of his professionalism is a certificate in dental surgery.
Other areas related to surgery
Surgical dentistry is closely related to other dental branches, without which it is practically powerless. Therapy, orthodontics, orthopedics, and pediatric dentistry create an information and practical basis for successful treatment and surgery.
It is also worth noting that any dental discipline is interconnected and intertwined with other medical areas:
- Therapy;
- Surgery;
- Ophthalmology;
- Radiology;
- Otolaryngology;
- and others.
Also, surgical dentistry is based on data from anatomy, diagnostics, physics and physiology, because the body is an integral and interconnected system.
Diagnosis and planning in dental practice
Before any surgical operation, careful diagnosis and proper planning are necessary. With this approach, you can accurately determine the features:
- location of the wisdom tooth germ and its root system;
- its fit to adjacent teeth;
- location of the maxillary sinus and mandibular nerve.
To obtain the necessary information, surgeons at the Bionic Dentis dental clinic use their own orthopantomograph. As a result, a full examination is carried out before tooth extraction and surgery planning. After removal, the success of the intervention and the absence of dental fragments are monitored.
Postoperative period
For complete healing of the mucosa after resection of wisdom teeth, it takes from 7 to 30 days. Recovery time depends on the complexity of the operation and the size of the existing wounds. To make this process as smooth and painless as possible, it is recommended to follow a number of rules:
- exclude traumatic factors - do not brush your teeth or rinse your mouth on the first day after the procedure
- For 7 days, when brushing your teeth, avoid direct contact with the wound;
- use only a soft toothbrush for hygiene;
- give up solid, spicy, hot and salty foods for 7-10 days;
- exclude physical activity - sports, bending, lifting weights;
- For the first time, limit taking hot baths, visiting baths, saunas - 3-4 days.
A few days after removal, the patient needs to see the attending physician.
At your follow-up appointment, the dentist will check how the gum surface is healing and rule out inflammation and possible complications. Pakhomova Anna Viktorovna Candidate of Medical Sciences, dental surgeon, periodontist, implantologist
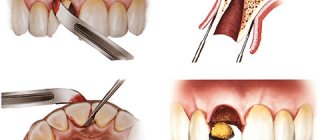
Modern method of tooth extraction
When removing a wisdom tooth germ using an outdated technique used in many Russian dentistries, a high degree of trauma is noted. The fact is that they perform the operation using powerful forceps, which severely damage the tissue adjacent to the tooth.
Modern methods of removing wisdom tooth buds allow the procedure to be performed in any convenient position, providing the patient with prompt and comfortable rehabilitation.
European specialists widely practice the method of removing wisdom tooth buds using ultrasound with the replanting of synthetic bone tissue and active regeneration proteins PRF.
Do I need to remove uncut “eights”?
Not all people develop their “8s” by the right age. Sometimes they remain in the anlage, that is, retained (not erupted). When to remove them:
- if on an x-ray we see that the wisdom teeth abut adjacent molars (seventh teeth). There is a risk that wisdom teeth will “eat” into an adjacent tooth inside the bone. And then you will have to remove 2 teeth.
- The pressure of the “eights” on neighboring teeth can cause caries of the root of the “sevens” - our main chewing teeth.
- If the wisdom teeth are large and there is no place for them in the oral cavity. There is a high risk that they will collide with the dentition, and a crowded position of the front teeth will appear.
- During implantation next to unerupted figure eights. It is worth removing the tooth so that it cannot damage the implant in the future.
The features of this highly effective technique used in the Bionic Dentis clinic are:
- The use of high-quality anesthesia, which completely eliminates any unpleasant and painful sensations during the procedure. If desired, all manipulations are performed in a dream.
- Removal of the wisdom tooth germ is performed using the PIEZOSURGERY ultrasonic system rather than forceps. Thanks to this, it is possible to avoid injury. If necessary, using an ultrasonic attachment, the tooth is separated from the bone tissue or divided into parts. This eliminates damage to adjacent tissues, nerves and blood vessels, as well as bone burns that occur when sawing bone with a drill.
- Sterilization of the tooth socket with a laser after extraction to prevent the formation of bacteria and infection.
- Injection of a synthetic bone preparation into the tooth socket for rapid restoration of damaged tissue. Clinic specialists use synthetic bone based on tri-calcium phosphate. This material, when compared with artificial bone of animal origin (from pigs or cattle), does not contain proteins that often cause rejection and the development of allergic reactions.
- Use of active PRF regeneration proteins obtained from the patient's blood. To do this, blood is first taken from a vein, which is processed using modern equipment installed in the clinic. You can get a blood regeneration protein drug that ensures 99% of synthetic bone engraftment in just 15 minutes.
- Place sutures at the extraction site to protect the socket from food and external irritants. This approach promotes rapid tissue healing, preventing the formation of swelling and the development of pain. This technique has no contraindications. It has been widely used for a long time in the USA and European countries, having proven itself only from the best side.
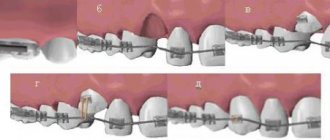
Extraction of individual teeth for orthodontic indications.
It is used as an independent method of treating dentofacial deformations and anomalies, as well as in combination with other methods. The correct choice of teeth to be removed allows you to achieve multiple stable contacts between the dentition and normalize the functions of the dentofacial system.
To determine the indications for the removal of individual teeth, a clinical examination, photographs and anthropometry of the face, the study of diagnostic models of the jaws, and radiography of the teeth, jaws, and skull are performed.
Based on a clinical examination and anamnesis data, the causes of dental anomalies and deformations, the age at which individual teeth were lost, the presence of bad habits, parafunctions and their duration are determined, if possible. If you are using mouth breathing, you should read the report of an otolaryngologist. The presence of anomalies of the dental system in close relatives and the transmission of certain characteristics (size of teeth, jaws) by inheritance are determined. For this purpose, the shape of the face, the size of the teeth, their location and the size of the jaws of the patient and his parents are compared.
The study of the shape of the face, the determination of its features associated with the incorrect arrangement of teeth, the development of dentoalveolar arches and jaw bones, according to indications, is supplemented with data from a photometric study of the face and an anthropometric study of the head. Photometric studies are carried out to identify the causes of dental anomalies. It allows you to significantly expand your understanding of the family characteristics of the size and shape of the face, facilitates diagnosis, drawing up a plan and determining the prognosis of treatment. The most valuable information can be obtained by examining the face in front and profile in children and their parents and comparing the data obtained. If a child has a narrower face than his parents (compare facial and morphological indices according to Isar), and the crowns of the teeth are larger than the average size, then in case of malocclusion this is one of the indications for the removal of individual teeth.
The similarities and differences in the shape of the face of children and parents are determined by comparing the shape of the polygons drawn on photographs of the face in front and profile according to Andresen. The magnitude of the convexity of the face or its concavity is compared based on the assessment of the angle of convexity according to Dons (n sn pg). When studying the face in profile, the size of the nose, the location of its root, the contours of the upper and lower lips, the shape and size of the supramental groove and chin are determined. This information is needed to determine indications for the removal of individual teeth in order to improve the shape of the face. If the nose is large, then there are fewer indications for removing teeth on the upper jaw, since the flattening of the upper lip due to the removal of individual teeth emphasizes the size of the nose, which is unfavorable from an aesthetic point of view.
When examining the dentition, the stage of bite formation is determined and the passport and dental ages are compared. It is advisable to remove individual teeth for orthodontic reasons during the period of mixed dentition and in the initial period of permanent dentition, i.e., at the age of 7 to 13 years. After tooth extraction at an older age, there are more indications for the use of fixed orthodontic appliances to close a dental arch defect.
Erupted supernumerary teeth during the period of breastfeeding must be removed. During the period of permanent dentition, well-developed supernumerary teeth, having a normal crown shape, located in the dentition, displacing and rotating the permanent teeth around their axis, can be preserved, and the complete teeth can be removed.
When deciding whether to remove teeth, the size and shape of their crowns are important. In children and adolescents, in the anterior section of the upper dental arch there are sometimes giant teeth, most often the upper central incisors, fused with the supernumerary ones. There are also ugly teeth with excessively large crowns or small, awl-shaped, vestigial shapes, most often the upper lateral incisors. In some cases they must be removed. It is important to assess the condition of the crowns of the teeth, the degree of their destruction, the possibility of restoration, the condition of periodontal tissues - inflammatory changes in the oral mucosa caused by the close arrangement of teeth, dysfunction of the dental system and other reasons.
In the case of congenital absence of the rudiments of individual teeth on one of the jaws (upper lateral incisors, second premolars, third molars), it is advisable to reduce the number of teeth on the opposite jaw. This treatment is called “leveling extraction.” They determine the type of anomalies in the position of individual anterior or lateral teeth, the lack of space for an incorrectly located tooth in the dental arch by '/4, 'D, '/.,, 3D of the width of its crown, the lack of space for a tooth with its medial (mesial) or lateral ( distal) side, as well as lack of space. It is necessary to clarify whether the close arrangement of the anterior teeth is due to a narrowing of the dental arches, individual macrodentia (discrepancy between the size of the teeth and the size of the apical base of the dental arches and the width of the face) or whether it arose as a result of mesial displacement of the lateral teeth and subsequent shortening of the dentition. It is important to find out whether there is a corpus displacement of the tooth in the dental arch or its tilt, as well as to determine the location of the tooth root. The decision about whether to remove a tooth should be made taking into account the way the adjacent teeth move. If these questions cannot be resolved on the basis of clinical examination, then they are clarified by evaluating data from further studies.
The study of diagnostic jaw models, especially gnatostatic ones, facilitates the establishment of indications for the removal of individual teeth. Measuring diagnostic jaw models involves determining the size of the teeth, dentition, areas of the dental arches and palate, and the ratios of various sizes.
On diagnostic models of jaws, it is possible to identify dentofacial anomalies caused by the close arrangement of teeth as a result of:
1) the presence of wide tooth crowns (usually the upper central incisors);
2) discrepancies in the sum of the width of the crowns of individual groups of teeth on one jaw or on both;
3) narrowing of the dental arches and their apical base;
4) mesial displacement of the lateral teeth.
If the teeth are closely spaced, then endo- and exogenous factors of such disorders are taken into account, including delayed jaw growth after the early loss of individual teeth.
When establishing indications for the removal of individual teeth, biological and genetic considerations are taken into account, and among the genetic ones, there is a discrepancy between the sizes of the base of the jaw and the crowns of the teeth, which can be observed as a result of disharmony during genetic recombinations.
The width of the crowns of the upper incisors is more variable than the width of the crowns of the lower incisors. The upper lateral incisors are among the rudimentary teeth, therefore the sum of the width of the crowns of the upper incisors is a more variable value than the lower ones, which is reflected in the calculated proper width of the dentition and the length of the anterior segment of the dental arches. In this regard, the use of the Tonn, Gerlach and Malygin indices in practical orthodontics makes it possible to identify the close position of the upper front teeth, caused by the disproportion in the sizes of the upper and lower incisors.
All teeth, teeth of one jaw, or separate groups of teeth may have abnormal sizes. If there is a discrepancy between the sizes of teeth and jaws, sequential tooth extraction according to Hotz is recommended. If there is a violation of the ratio of the sizes of the upper and lower teeth (more often this applies to the group of incisors), individual teeth on one jaw are removed. Removal of individual teeth is indicated in cases where, when the anterior teeth are closely spaced, the central incisors are wider than 10 mm, and the lateral incisors are wider than 7.5 mm, when the narrowing of the dentition in the area of premolars and molars exceeds 6 mm, the narrowing of its apical base is 5 mm, in cases where the sum of the width of the crowns of the upper incisors is 35 mm or more. However, with a narrow face, the sum of the width of the upper incisors exceeding 33 mm may be a sign of individual macrodentia, in which the removal of individual teeth is indicated in order to eliminate malocclusions.
Noteworthy is the ratio of the width of the dental arch and its apical base. Expansion of the dental arch with a narrow apical base leads to vestibular deviation of the teeth, and, consequently, to disruption of the correct transmission of chewing pressure on the teeth, disruption of tooth articulation and subsequent relapse. According to A. Howes, confirmed by N.G. Snagina, the percentage ratio of the sum of the width of the crowns of the 12 upper and 12 lower teeth and the apical bases of the dental arches makes it possible to judge the degree of narrowing of the apical base and objectively decide the issue of indications for the removal of individual teeth.
The choice of teeth to be removed can be made after assessing the dentition and their closure in three mutually perpendicular directions. The size of the sagittal gap between the incisors, the presence of the usual displacement of the lower jaw forward, to the side, as well as the depth of the incisal overlap or the severity of the open bite are determined. They identify dysfunctions of breathing, swallowing, speech, chewing, and determine the characteristics of the movements of the articular heads in the articular sockets in order to resolve the issue of the possibility of eliminating these disorders after the removal of individual teeth and normalization of the bite.
An X-ray examination reveals supernumerary teeth, adentia (including upper lateral incisors, second premolars, third molars), assesses the size of carious defects in the crowns of teeth, the condition of their periapical tissues, and in the case of retention of individual teeth - the location of their rudiments (correct - in the direction of eruption or incorrect), the degree of formation of crowns and roots of tooth buds and anomalies of their shape, the degree of resorption of the roots of primary teeth, the ratio of the roots of primary teeth and the crowns of permanent teeth. Particular attention is paid to the condition of the first permanent molars, the position of the canines and their buds, the inclinations and displacements of these teeth. The location of the canine primordia is determined, which helps to decide the issue of removing fangs, first premolars or lateral incisors, especially in cases of resorption of their roots under the pressure of incorrectly located canine primordia. For this purpose, intraoral close-focus radiographs of the teeth and alveolar processes, panoramic photographs of the jaws or their orthopantomograms are studied.
Comprehensive diagnostics, including, if indicated, a clinical examination of patients, facial photometry, examination of diagnostic models of the jaws, radiographs of the teeth, orthopantomograms of the jaws and lateral TRGs of the head, makes it possible to clarify the indications for the removal of individual teeth in order to normalize the bite. The question of choosing teeth to be removed should be decided individually, taking into account the periods of growth and development of the dental system.
LJ Baume studied the displacement of adjacent teeth after the removal of the first molars and first premolars and described its patterns. They are as follows:
1) after early removal of the first permanent molars, the adjacent teeth move corpusally towards the defect: premolars - distally, second molars - mesially;
2) on the upper jaw, teeth move faster than on the lower jaw;
3) erupting premolars move distally more slowly than the second molars move mesially.
The reasons for non-simultaneous movement of teeth, according to LJ Baume, are as follows:
1) tooth buds shift towards the removed tooth faster than erupted teeth and teeth established in occlusion;
2) tooth displacement accelerates during the eruption of teeth located one or two teeth apart from the removed one;
3) teeth with unformed roots move faster than teeth with fully formed roots.
In 1919, it was proposed to remove first the primary canines to correct the position of the incisors, and then the first premolars to correct the position of the canines, which was called “sequential extraction.” R. Hotz called this activity “teething management by extraction.” The effectiveness of this method of treatment was confirmed by G. K. Spataru, F. Ya. Khoroshilkina, V. P. Norkunaite, N. Briickl, V. E. Dewel, S. F. A. Moorrees and others. R. Hotz recommended controlling teething mainly with Angle class I anomalies (Fig. 19.4)
, and subsequently with sagittal malocclusions, open and cross bites.
Rice. 19.4. Sequential removal of upper and lower teeth according to Hotz. and (1-4) - with a neutral occlusion.
Rice. 19.4. Continuation. b (1-4) - with mesial bite and partial grinding of crowns
upper second primary molars in order to normalize the closure of the teeth
rows.
Consecutive removal of individual teeth or their groups includes the following measures: 1) removal of temporary canines in case of improper eruption of the lateral incisors. In this case, self-regulation of the position of the lateral incisors occurs as a result of the use of massage, or their position and malocclusion are corrected with the help of orthodontic devices;
2) removal of the first temporary molars when the rudiments of the first premolars approach the surface of the alveolar process, which accelerates their eruption; 3) removal of prematurely erupted first premolars, which helps to change the location of the rudiments of permanent canines and their correct installation in the dentition. If, based on radiological control, the eruption of the second premolar can be expected earlier than the first, then the first premolar should not be removed, since this will result in an undesirable mesial displacement of the second premolar and the first permanent molar, as a result of which the space for the canine in the dental arch is reduced. In such cases, the first premolar must be removed after the second premolar has been established in the dental arch and before the eruption of the canine. If the eruption of the canine can be expected before the eruption of the second premolar, then the first premolar should be removed more quickly in order to create conditions for the correct establishment of the canine in the dentition; 4) observation of the eruption of canines and second premolars and their establishment in the dentition.
Sequential removal of individual teeth to control the eruption of others is indicated under the following conditions.
1. Absolute macrodentia, when the sum of the width of the crowns of the 4 upper incisors (SI) is 35 mm or more, and the lower ones (Si) is 27 mm or more, the front teeth are closely spaced, there is no space for two or more teeth in the dental arch or not enough for up to '/2 the width of their crowns, the face is narrow or of medium width. If the relationship between the canines and first permanent molars is neutral and the anterior teeth are closely spaced, it is advisable to remove individual teeth on both the upper and upper teeth. and on the lower jaw, with a distal bite usually on the upper jaw, with a mesial bite - on the lower jaw.
2. Relative (individual) macrodentia, when SI = 33-34 mm, Si = 26-27 mm, the face is narrow, long, there is no space for two teeth (usually lateral incisors) on each jaw or it is missing by '/2 of the width their crowns, as well as when the teeth are closely spaced and the face of the parent the child resembles is narrow. With a neutral relationship of the lateral teeth, sequential removal of teeth on the upper and lower jaw is indicated.
3. Significant discrepancy between the sizes of temporary molars and premolars on one or both jaws and a violation of the closure of the lateral teeth (II or Angle’s class), requiring grinding of the proximal surfaces of the crowns of temporary canines and molars to ensure mesial shift of the first permanent molars and achieve a neutral occlusion, which is not eliminates sequential removal of individual teeth.
4. Early loss of primary teeth, multiple carious destruction of the proximal surfaces of their crowns and subsequent shortening of the dentition by 4 mm or more as a result of mesial movement of the lateral teeth.
5. The mesial inclination of the canine and premolar buds is from 35° or more relative to the median plane, determined by studying orthopantomograms of the jaws, and the close arrangement of the incisors.
6. Underdevelopment of the lower jaw, excessive development of the upper jaw with distal occlusion with protrusion of the upper anterior teeth and questionable results of orthodontic treatment. When planning the treatment of such patients with a sagittal gap between the incisors, it is advisable to use clinical functional tests by Ilina Markosyan, Eschler-Bitner, etc. with the displacement of the lower jaw forward to a neutral relationship of the first permanent molars. If, after protrusion of the lower jaw, the shape of the face deteriorates, then the distal bite is caused by the mesial displacement of the lateral teeth. In such cases, it is necessary to either move the lateral teeth distally or remove individual teeth in the upper jaw in sequence.
7. Underdevelopment of the upper jaw, excessive development of the lower jaw, mesial bite without displacement of the lower jaw, questionable prognosis for treatment. Sequential removal of individual teeth in the lower jaw is indicated.
8. Open bite in combination with close arrangement of the front teeth, insufficient space for them, hypoplasia of the enamel of the incisors and molars. Sequential tooth extraction is indicated in combination with the use of orthodontic appliances and training with a speech therapist.
If there are orthodontic indications for the removal of individual teeth on the right and left halves of the jaws, it is advisable to remove them simultaneously or with an interval of up to 1 month to avoid displacement of the midline between the incisors. After the removal of individual teeth, massage of the alveolar process is indicated, which accelerates the eruption of permanent teeth. The relationship of teeth on the right and left sides of the jaws is not always the same.
The Hotz method is used independently or in combination with orthodontic. Its disadvantage is the need for long-term (3.5-4 years) monitoring of the patient. This method should not be used when treating fearful and undisciplined children. In such cases, treatment can be delayed until the age of ten. By this period, temporary canines and first temporary molars fall out, the first premolars begin to erupt, which can be removed and thereby speed up treatment. However, after the removal of the first premolars, the use of orthodontic appliances is indicated for anomalies in the position of the incisors and vertical malocclusions (Fig. 19.5).
Rice. 19.5 Contours copied from ortholantomograms of patient K’s jaws.
In the final period of the mixed and permanent dentition, it is generally recommended to remove the first premolars. They rank first in terms of frequency of removal for orthodontic treatment; second place belongs to the first molars. Second and third molars are rarely removed.
For the purpose of orthodontic treatment, it is possible to remove teeth on one or both jaws, teeth located symmetrically and asymmetrically. A combined removal of individual premolars, molars, incisors or other teeth is performed. In the case of partial congenital absence of the rudiments of individual teeth, after tooth loss due to caries, its complications or trauma, “leveling extraction” is recommended. The best results are achieved with symmetrical removal of teeth of the same name. The removal of individual teeth should be approached individually, taking into account the above features.
Ultrasonic removal of wisdom tooth germ
The use of synthetic bone of non-animal origin, the use of active prf regeneration proteins, the European protocol for the sterility of instruments in the clinic, high qualifications and extensive experience of the dental surgeon, thorough diagnosis and planning of removal using our own orthopantomograph.
In Moscow dental clinics, the method of removing wisdom teeth with bone grafting has not yet become widespread. To fully implement it, expensive equipment and materials are required. Namely:
- dental laser;
- PIEZOSURGERY device;
- synthetic bone preparations and PRF.
In addition, since 2006, dental surgeons from the Bionic Dentis clinic (Moscow) regularly undergo training in Germany on modern surgical techniques for removing wisdom tooth buds. For further work using the new method, the clinic purchased the necessary high-tech equipment.
During this time, specialists have helped more than 1000 patients with various wisdom teeth problems. A new technique for removing wisdom tooth buds with bone grafting at the Bionic Dentis clinic allows patients to recover quickly, go back to work the next day and lead a normal lifestyle. Many years of experience show that the recovery period is reduced by 3 times compared to the conventional method.
Modern dentistry in Western countries is developing in the direction of microinvasiveness and atraumaticity. The use of high-quality artificial bone preparations, lasers and high professional training of doctors allows us to completely eliminate unpleasant sensations and speed up the rehabilitation process during any interventions.
Expert commentary
Ozerov Petr Vladimirovich, dental surgeon, implantologist. Expert implantologist at BIOTECH (France) in the Russian Federation. Chief physician of the dental clinic.
“Removing the wisdom tooth germ using a unique technique using ultrasonic bone surgery PIEZOSURGERY allows you to avoid tissue trauma. This procedure is quick, as is the subsequent recovery. The use of active regeneration proteins PRF with the grafting of synthetic bone tissue is practiced by European dentists at business class clinics. Now the new method is available to patients of the Moscow dental clinic “Bionic Dentis”. Therefore, removal of wisdom teeth in our patients is completely painless, and recovery is 3 times faster!
Ozerov Petr Vladimirovich
Chief physician. Dentist, implantologist, orthopedist, surgeon. Laser dentistry specialist
More details
Frolov Andrey Konstantinovich
Orthopedic dentist
More details
Andreev Dmitry Lvovich
Dentist orthopedist-implantologist.
More details