A. Iandolo, Doctor of Dentistry, Professor
One of the main reasons for failure in endodontic treatment is the inability to localize and treat the entire root canal system, resulting from a lack of knowledge of the internal or external anatomy of the tooth, as well as due to the high complexity and variability of the system, including the presence of subsidiary canals and apical deltas. The molars of the upper jaw are the teeth with the largest number of roots of various shapes, so their canal system is very variable.
Various studies have shown large variations in the detection of the MB2 canal in the maxillary second molar: in in vitro studies its occurrence varies between 29% and 100%, in vivo - 19.7% and 51.1%. Traditionally, most endodontic procedures for canal locating relied on the dentist's sense of touch and understanding of the canal system because the ability to visualize the orifice was severely limited. By enlarging and illuminating the orifices, and differentiating differences in the color of the dentin of the bottom of the pulp chamber and the walls of the canals, the operating microscope made the search easier.
The use of magnification during endodontic treatment significantly reduces the risk of perforation, and also allows you to effectively search for the MB2 canal, which leads to an increase in the number of such canals. The goal of endodontic therapy is the adequate formation, proper cleansing, followed by obturation, of a complex root canal system. Hand and machine instruments do not have full contact with the canal walls, for this reason, after shaping, more force must be applied during the cleansing stage.
Using modern 3D cleaning techniques, all areas and undercuts can be treated. Even if complete removal of bacteria is not achieved, the number of bacteria will be small enough to allow the defense mechanisms to work and achieve good results in the short and long term. A significant percentage of failures occur due to the presence of pulp residues. Thanks to knowledge of canal anatomy and its possible variations, as well as modern technologies, it is possible to find all root canals and achieve greater control at each stage of treatment.
Upper central and lateral incisors
The contours of the intradental cavities are similar in these teeth. The central incisors are large, on average 23 mm in length (span 18-29 mm). The lateral incisors are shorter - 21 - 22 mm (span 17-29 mm). The shape of the canals is usually type I and it is extremely rare in these teeth to have more than one root or more than one canal. If abnormalities exist, they are usually in the lateral teeth, and may present as an accessory root (dens invaginatus), duplication or fusion of roots (Shafer et al., 1963).
The pulp chamber on the vestibulo-oral incision narrows towards the cutting edge and widens at the level of the cervix. Mediodistally, the pulp chambers of these teeth follow the contours of their crowns and the widest space at the incisal edge. Central incisors in young patients usually have three pulp horns. The laterals usually have two horns and the contours of the intradental chamber tend to be more rounded than in the central incisors.
Upper first incisor
The dotted line indicates the contours of access to the intradental cavity. Gray indicates the contours of the intradental cavity in young people, black in old people. Two sections of the root are shown:
1 - 3 mm from the apex,
2 - at the level of the canal mouth. (By Harty).
In the vestibulo-oral projection, the canals are much wider than in the mediodistal, and often have a narrowing just below the level of the neck of the tooth. Typically, textbooks indicate that the coronal cavity in these teeth directly passes into the root canals. However, this narrowing is largely reminiscent of the orifices in multi-rooted teeth. This narrowing, as a rule, is not visible on an x-ray, but it should be taken into account when instrumenting the canals (it is better to open it with a spherical bur at low speeds).
The canals of the upper incisors taper towards the apex and are initially oval or irregular in shape at the neck, which gradually becomes round towards the apex.
There is usually very slight apical curvature in the central incisors toward the distal or labial sides. The apical part of the lateral incisor is often curved, usually in the distal direction.
Upper second incisor
The frequency of occurrence of lateral (lateral) canals in central incisors is 24%, in lateral incisors - 26%, and the frequency of deltoid branches (additional canals) in central incisors is about 1%, in lateral incisors - 3%.
The apical foramen in the central incisors in 80% of cases is located at a distance of 0-1 mm from the radiographically determined root apex, in 20% of cases - at 1-2 mm. In lateral incisors, in 90% of cases these ratios are from 0 to 1 mm, in 10% - from 1 to 2 mm. With age, the anatomy of the intradental pulp changes due to the deposition of secondary dentin, and the roof of the pulp chamber may end up at the level of the neck, although in young teeth the roof of the pulp chamber reaches 1/3 of the length of the clinical crown of the incisors. A mediodistal radiograph may show significant narrowing. However, it must be remembered that the canal is wider in the labio-palatal direction, so it can often be passed through relatively easily, although on the radiograph it appears very thin or not visible at all.
How is root canal treatment performed?
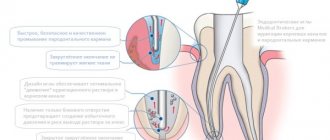
An important step in the process of treating root cavities is determining the working length of these canals. Not everyone knows the definition of tooth root length. So, the working length of the root canal is the distance from the edge of the frontal units to the apical constriction preceding the apical foramen. There are several methods for determining the working length of the root canal. The most commonly used are the calculation method, x-ray and electrometric methods.
Endodontics treats tooth root canals. When an endodontist treats a root canal, he performs the manipulations in the following sequence:
- diagnostics,
- x-ray,
- preparing the dental cavity for treatment,
- anesthesia,
- chemical treatment of instruments,
- opening of the tooth cavity,
- determination of the working length of root canals,
- medicinal treatment, cleaning and expansion of root canals along the entire working length,
- filling a tooth cavity.
READ ALSO: What should be the sequence and pattern of teething for children?
Diagnostic methods
The first stage of tooth root canal treatment is diagnosis, which will help the doctor make the correct diagnosis and decide on a treatment method. To do this, the patient needs to undergo an x-ray to examine the part of the crown that the doctor cannot see. This procedure allows you to understand how many roots and canals the tooth cavity has. If the X-ray examination is ignored, then the cavity of the diseased tooth will have to be opened again (we recommend reading: X-ray of a child’s jaw: is it possible to take an X-ray with baby teeth?).
INTERESTING: How many teeth should an adult healthy person have?
Preparatory procedures
After the X-ray of the dental cavity has been carefully studied, the diagnosis has been made, and the stages of the upcoming therapy have been planned, it is necessary to tell the patient about everything in detail. Next, you need to obtain documented consent for the opening and further treatment of the tooth cavity.
An important point in preparing for root cavity treatment is for the doctor to obtain information about the presence of allergic reactions in the patient to anesthetics. If such information is not available, an allergy test is performed. At this stage, chemical treatment of the instruments with which the manipulations will be performed is carried out.
Administration of anesthesia and application of anesthetic
Before treatment begins, the patient is anesthetized in the area of the jaw where the intervention will be performed. Anesthesia can be superficial or in the form of an injection. The first type of anesthesia blocks sensitivity not only in the dental cavity, but also on the mucous membrane. It is usually used to numb the area where the doctor is about to inject an anesthetic.
The following drugs are used for superficial anesthesia:
- 0.5% Promecaine ointment,
- Anestezin,
- Lidocaine,
- Dicaine.
Opening a molar tooth
What is the opening of a tooth cavity? In order to remove the pulp and clean the root canals, the dentist needs to provide good access to them. Opening the tooth cavity can begin immediately after grinding the caries and removing sawdust from the dentin. The process of opening the tooth cavity begins with the smallest bur, after which a large spherical one is used.
INTERESTING: the structure of the human oral cavity and the functions of the organs that are located in it
Medicinal treatment of canals
Canal treatment is divided into mechanical (scraping out the contents using special tools) and chemical (medicinal treatment of root canals with disinfectants injected with a thin needle). Today, the following scheme for medicinal treatment of the root canal is used: sodium hypochloride is applied after using each instrument and completing mechanical cleaning, then hydrogen peroxide, and after that distilled water. Drug treatment of root canals is carried out immediately after the opening of the dental cavity is completed.
Sealing
The final stage of tooth root canal treatment is sealing the cavity. The root cavities are filled with a special filling material (usually gutta-percha). The filling helps the tooth remain strong and prevents pathogenic bacteria from entering its cavity.
Filling a tooth cavity can be:
With temporary filling, the tooth cavity is filled with a non-hardening paste that has medicinal properties. This type is used in cases with advanced three-channel pulpitis or periodontitis. If there is no sign that there is inflammation in the tooth cavity, then removal (for example, the 6th) is not carried out, and a permanent filling is installed. In this case - without consequences.
Upper canine
It is the longest tooth in the mouth, averaging 26.5 mm (range 20-38 mm). It is extremely rare to have more than one root canal. The pulp chamber is relatively narrow and has only one horn; it is much wider in the vestibulo-oral section than in the mediodistal section. The root canal is type I and becomes round only in the apical third. The apical constriction is not as pronounced as in the incisors. This fact, and the fact that often the apical part of the root is significantly narrowed, causing the canal to become very narrow at the apex, makes it difficult to determine the length of the canal.
Upper canine
The canal is usually straight, but sometimes at the apex it bends towards the distal (in 32% of cases) and, less often, the lateral side. In 13% of cases, vestibular deviation of the canal was recorded. The frequency of occurrence of lateral (side) canals is about 30%, and additional apical ones - 3%. The apical foramen is located in 70% of cases in the range from 0 to 1 mm in relation to the root apex, and in 30% in the range of 1 - 2 mm.
Can three-channel pulpitis go away on its own?
Pulpitis of a three-canal tooth, of course, will not go away from lack of treatment and will become chronic. The nerve will die under the influence of microbes, the pain will go away, and the patient will deceptively think that the problem is solved. But this will turn out to be a temporary calm before the storm. The nerve will decompose inside the tooth, there will be even more microbes, inflammation will affect the surrounding tissues, and ultimately it will all end in the formation of a cyst. It will be very difficult to save such a tooth from removal. Treatment of pulpitis of a 3-canal tooth should be immediate.
Access to the canals of the upper incisors and canines
The access may vary in size and shape depending on the size of the pulp chamber. It should be such that the instruments can reach the apical constriction without bending or obstruction by the canal walls.
If access is too close to the cingulum, this will result in significant bending of the instruments and possible perforation or staircase formation.
An incorrectly formed access cavity in the incisors and canines leads to the formation of a ledge on the labile surface of the canal due to a sharp curvature of the instrument in the canal. This approach leads to failure to remove remaining pulp.
Ideally, the access should be close enough to the incisal edge to allow unimpeded entry of instruments to the apex. Sometimes the cutting edge and labial surface of the tooth are involved in the access (see figure). At first glance, this is contraindicated from an aesthetic point of view. However, if the root canal is not fully processed, it will not ensure long-term health of the periodontal tissues.
Access to the upper incisors: a) view from the palate; b) side view.
On the other hand, modern whitening and restorative techniques make it possible to ensure aesthetics, strength and other requirements in restoring these defects.
Because the pulp chamber is wider at the incisal edge than at the neck, the access contour should be triangular and sufficiently extended medially and distally to include the pulp horns. With proper access, it is necessary to widen the cervical narrowing for adequate instrumentation of the canal.
Access contours in incisors:
a) correct access contours in the incisors and canines; b) the dotted line shows an incorrect access contour in which infected material can remain in the pulp chamber and be pushed into the canal during further instrumental processing. (by Harty)
Correct access is especially important in older patients, as a narrowed canal requires thinner instruments that can bend sharply or even break. In such patients, it is better to immediately make access closer to the cutting edge than usual, since due to the narrowing of the pulp chamber, a straight line of transition of this chamber into the canal is formed. This will ensure effective preparation.
Access contours in the upper canine.
Process and stages of root canal treatment
The root canal treatment process has a clear sequence of stages:
- Initially, it is necessary to correctly diagnose the disease. In difficult cases, the dentist sends the patient for an x-ray.
- After this, the doctor carries out the necessary preparatory procedures in the oral cavity for treatment.
- Canal treatment is a rather painful procedure, so the tooth must be numbed by injecting anesthesia (usually into the gum near the diseased tooth).
- After this, complete asepsis of all instruments is carried out and the diseased tooth is separated from the rest using a special rubber film (caffedram).
- Next, the diseased tooth is opened using a drill, providing maximum access to the diseased canals, after which they are initially cleaned, the infected pulp is removed, and in parallel the canals are treated with special medications.
- Afterwards I dry them and seal them with special materials.
If the doctor has any doubts (usually this happens when the tooth is inconveniently positioned and instruments have difficulty accessing it), he puts a temporary filling , after which he sends the patient for an x-ray, using a photo of which he checks whether all the infection has been removed and whether all the canals have been removed. cleaned it. The permanent filling is then placed approximately two weeks later.
This whole procedure, of course, is not very pleasant, but it allows you to save the tooth. Its duration depends on the location of the tooth, the number of canals in it, the complexity of the developed infection and usually takes from thirty minutes to one hour. And success depends on the professionalism of the doctor and the high-quality work he has done, since it is necessary to remove all the affected pulp from the canals without leaving a drop of infection, otherwise it can develop again and tightly seal the tooth so that nothing else can get into the cleaned cavity.
Upper first premolar
Upper first premolar with two roots
Typically these teeth have two roots and two canals. The frequency of occurrence of the variant with one root, according to the literature, is from 31.5% to 39.5%.
These data show the ratio for people of Caucasian descent. In Mongoloids, the frequency of these single-rooted teeth exceeds 60% (Walker, 1988). One study (Carns and Skidmore, 1973) found 6% of teeth had three roots. A typically Caucasian tooth with two well-developed roots that separate in the middle third of the root. In Mongoloids, root fusion prevails.
Possible morphology of the roots of the upper first premolar in transverse sections
This tooth usually has two canals and, in the case of a single-rooted variant, these canals can merge and open into one apical foramen. These teeth show many types of canal configurations and the presence of lateral canals, especially in the apical region - 49.5% (Vertucci and Geganff, 1979). The three-root version has three canals: two buccal and one palatal.
Typically, the average tooth length is 21 mm, which is shorter than the second premolar. The pulp chamber is wider in the bucco-palatal direction with two clearly distinguishable horns. The bottom of the chamber is rounded, with the highest point in the center and usually just below the level of the cervix. The mouths of the canals are funnel-shaped.
With age, the size of the pulp chamber mainly decreases due to the deposition of secondary dentin on the roof of the pulp chamber, which causes the roof of the cavity to become closer to the bottom. The bottom remains below the level of the neck and the roof, due to dentin deposition, may also be below the level of the neck.
The canals are usually separated and very rarely merge, taking on a ribbon-like shape characteristic of the second premolar. They are usually straight and round in cross section.
Sixth tooth from bottom
There are no two identical root dental systems, which is explained by the purely individual structure of a person’s teeth. In addition, the root system of incisors, canines and molars is arranged in accordance with their purpose:
- Ones and twos (incisors) are needed for biting food.
- Fours and fives (premolars) perform the initial chewing function.
- Sixes and sevens completely grind food.
Based on this, it becomes clear that the seventh tooth requires more nutrients than the fifth. It must be strong and hardy, therefore it has a more developed channel system.
Despite the fact that the 6th tooth in the lower jaw performs the same functions as the seventh, it usually has fewer canals.
This is due to the fact that there is less chewing load on it.
For a detailed study of the structure of the dentofacial apparatus of a particular patient, radiographic examination is used.
Tooth structure
Each dental unit consists of:
- crowns - the area above the gum;
- neck - the area between the crown and the root;
- root - the area under the gum.
Inside the crown is the pulp, which passes into the root canals. At the end of the root there is a small apical opening through which blood vessels and nerve endings pass, starting from the main neurovascular bundle and ending in the pulp.
When a person’s pulp becomes inflamed, not only it, but also all root canals need to be cleaned of infected tissues, since they are “communicating vessels.” If even one canal is left uncleaned, pathogenic microorganisms will continue to develop inside the dental unit, which will lead to its removal. That is why the doctor must know the exact number of canals in the tooth.
Thanks to the nerve, the tooth can respond to external stimuli. After removing the pulp and filling the canals, the dental unit loses sensitivity, as it is deprived of a nerve.
But due to the removal of blood vessels, problems begin with its blood supply and mineralization. The crown becomes less durable and more prone to various chips and breaks.
The enamel quickly darkens, and it cannot be properly bleached even with strong chemicals.
Before removing the pulp, the patient is sent for an x-ray to find out how many canals are in the operated tooth: a person has only one dental nerve in a tooth, but there may be several canals. This preparation allows for depulpation to be carried out competently and quickly.
There are several options for the structure of dental canals:
- in the root there is one canal passage, which corresponds to one apical foramen;
- in the root there are several canal branches that connect in the area of a single apical foramen;
- two different branched passages have one mouth and two apical openings;
- canal cavities in one root merge and diverge several times;
- three root canal passages emerge from the same orifice, but have 3 different apical openings.
There can be as many channels as there are roots, but often their number differs. Several types of canals may be present in one molar and premolar.
According to statistics, the number of canals depends on the depth of the tooth: the deeper it is located in the jaw, the more canals it has. This is due to the increased load on the molars located at the base of the dentition.
The table below presents average statistical data on how many canals are in a person’s teeth above and below.
Dental unit Number of canal passages
| Fangs | Upper | 1 | |
| Lower | 2 | ||
| Incisors | Upper | 1 | |
| Lower | Central | in most cases 1, less often 2 | |
| Lateral | 1 or 2 (about the same probability) | ||
| Premolars | Upper | First | most often 2, but sometimes first premolars with 1 or 3 canals are found |
| Second | in most cases 2, sometimes 1 or 3 | ||
| Lower | First | 1 or 2 | |
| Second | 1 | ||
| Molars | Upper | First | 3 or 4 with equal probability |
| Second | in most cases 3, sometimes 4 | ||
| Third | around 5 | ||
| Lower | First | most often 3, sometimes 2 or 4 | |
| Second | usually 3, but there are roots with 4 channels | ||
| Third | no more than 3 |
The tooth root is located in the inner part of the gum. This invisible part makes up about 70% of the entire organ. There is no clear answer to the question: how many roots does this or that organ have, since their number is individual for each individual patient.
Factors influencing the number of roots include:
- organ location;
- degree of load on it, functional features (masticatory, frontal);
- heredity;
- patient's age;
- race.
Additional Information! The root system of representatives of the Negroid and Mongoloid races is somewhat different from the European one; it is more branched, which, in fact, is the reason for the larger number of roots and canals.
Dentists have developed a special system for numbering teeth, thanks to which it is almost impossible even for a non-specialist to get confused in the units of the upper and lower dentition. To understand the principle of numbering, you need to mentally divide the skull in half vertically. First come the incisors - the frontal units of the upper and lower rows on the right and left.
There are two of them on each side: central (No. 1) and side (No. 2). Next come the fangs or so-called triplets. The four (No. 4) and five (No. 5) are the first and second premolars. These teeth are also called small molars. All of the above units are united by the fact that they have only one cone-shaped “spine” in both the top and bottom rows.
The situation is somewhat different with the first, second and third molars, we are talking about tooth No. 6, 7 and 8. The upper six and seven (large molars) are endowed with three roots, however, in the wisdom tooth located on top, as a rule, there are also 3 grounds. The sixth tooth and the 7th tooth of the bottom row usually have one less root than their upper counterparts.
How many canals does a wisdom tooth have?
The number eight or the so-called third molar is somewhat different from other units of the dentition. To begin with, it should be noted that not all people have it, which is due to genetic factors.
This organ, in addition to its inconvenient location, which causes discomfort during oral hygiene, has other differences. Thus, the upper third molar is the only unit whose number of canals can reach 5. It is worth noting that this happens extremely rarely, mostly wisdom teeth have three or four canals. The bottom eight has no more than 3 indentations.
Number eight is often the cause of the development of dental pathologies. For example, incorrect placement of the third molar can contribute to impaired growth of adjacent units.
In such cases, its removal is required. If the figure eight does not bother or hurt, there is no need to pull it out.
The only indication for removal is the presence of pain and the negative impact of the third molar on other units of the row.
To avoid problems with the figure eight, dentists advise adhering to the following rules of oral care:
- due to the inconvenient location of the figure eight, it is necessary to use a special brush;
- Owners of a third molar should visit the dentist for a routine examination at least 2 times a year.
Channels in baby teeth
There are as many nerves in baby teeth as there are in molars—one. In addition, temporary units are similar to permanent ones in the structure of the root system. That is, a milk tooth such as the upper six or second molar has a canal system similar to its molar brother, the second premolar.
Nerve endings perform standard functions:
- signal about developing caries;
- responsible for the growth and development of teeth;
- control the flow of water and nutrients to dentin and enamel.
The root canals of baby teeth are also treated and filled, but the tactics of their treatment depend on how long ago they erupted. Under the temporary units, permanent ones are formed, so treatment should be aimed at preserving them. Milk teeth can only be removed if the permanent teeth are ready to emerge.
The roots of permanent incisors, canines and molars do not form immediately, but over the course of about 3 years. Treatment of permanent teeth with unformed roots also differs from the standard one. The canals in the teeth of patients four, five, six years old (depending on the rate of formation of the dentoalveolar apparatus) are filled with a special paste with calcium and fluoride, which helps close the roots.
Root canal treatment
Root canals can become inflamed due to the development of the following diseases:
- caries;
- pulpitis;
- periodontitis.
An accurate diagnosis of inflammation of the pulp and canals of the tooth can only be determined by a dentist after X-ray diagnostics and a visual examination of the oral cavity.
The treatment plan for dental canals consists of several stages:
- First, access to the problem area is freed: using a special dental instrument, the filling or the area of the crown damaged by caries is removed.
- Then the contents of the pulp are removed, and the canals are cleaned mechanically using antiseptic drugs.
- After this, the root is prepared for filling. At this stage, the dentist can form the correct conical shape of the canal passage.
- Then the canals are carefully sealed. If baby teeth are treated, the dentist uses a special filling paste, which gradually dissolves as the root dissolves.
- After this, a filling is placed on the crown.
This treatment regimen is standard and does not depend on exactly how many canals there are in the diseased tooth. The main thing is that all dental canals are cleaned, treated with an antiseptic and carefully closed. If treated incorrectly, it may be necessary to remove the tooth and visit an oral surgeon.
Teeth can be single-channel, two-channel, three-channel and even eight-channel. If one of the ducts becomes inflamed, it is necessary to clean and seal not only it, but also all other canals, since the infection could penetrate into them.
The development of dental pathologies can be prevented only by following the advice of qualified doctors and observing the rules of oral hygiene.
So, for prevention purposes, dentists recommend:
- do not abuse the rules of hygiene, brush your teeth only in the evening and in the morning. More frequent exposure to tooth enamel contributes to its wear;
- hygiene procedures should be carried out half an hour after eating;
- use rinses to destroy germs remaining in the mouth after brushing;
- Cleaning should be carried out for at least 3 minutes, performing circular movements.
The main rule is that if the first signs of the disease are detected, you should immediately contact your dentist. This will help prevent further development of pathology and preserve teeth.
Each dental unit has its own functions, depending on its structure and location on the jaw. Thus, incisors are designed for biting off pieces of food, canines help to hold hard food and “tear off” stubborn pieces, premolars are needed for primary processing, and dense “plump” molars are designed for thoroughly chewing and grinding food.
the upper right is the first and is indicated by a ten in front of the number of a particular tooth (for example, the 11th is the central right upper incisor, the 16th is the upper right molar, immediately following the premolars, etc.
), top left – twenty. Accordingly, the lower left is designated by thirty, and the lower right by the number 40.
That is, the segments of the jaws are numbered clockwise, so it is much easier to remember the order and, if necessary, count.
Thus, the notorious 48th number indicates the location of the wisdom teeth in the lower right segment of the jaw. And insisting on removing the 48th dental unit, the dentist simply indicates what number the wisdom tooth has in the lower right, and does not inform the patient about the supernumerary teeth that came from nowhere in the mouth.
Source: https://smile-nn.ru/blog/shestoy-zub-snizu/
Upper second premolar
Upper second premolar. (I channel configuration type).
This tooth tends to be single-rooted. Type I of the canal configuration prevails, but in 25% types II and III are present, and in 25% there may be types IV - VII with two apical openings.
Thus, the basic type of this tooth can be considered as single-rooted with a single canal. Rarely, there may be two roots, and then the tooth resembles a first premolar with the bottom of the cavity located significantly below the neck of the tooth. The average length is slightly longer than the length of the first premolar and averages 21.5 mm.
The pulp chamber is expanded in the bucco-palatal direction and has two pronounced horns. Compared to the first premolar, the bottom of the chamber is located closer to the apex.
The root canal is wider in the bucco-palatal direction and narrower in the mediodistal direction. It tapers towards the apex, rarely round in cross-section, with the exception of two or three mm at the apex. Often the root of this single-rooted tooth is divided into two sections by a groove in the middle third of the root. These sections are connected almost without variations and form a common canal with a relatively large apical opening. The canal is usually straight, but the apex may have a curvature distally and, less commonly, buccally.
With age, the displacement of the roof of the pulp chamber is the same as in the first premolar.
Upper first molar
Contours of access to the upper premolars.
This tooth usually has three roots and four root canals. Additionally, the canal is located in the mediobuccal root. The shape of the channel system was studied both in vivo and in vitro. In in vitro studies, an additional channel was found in 55–69% of cases. The canal configuration is usually type II, but type IV with two separate apical foramina is present in more than 48.5% of cases. In in vivo studies, an additional second channel was less frequently found and there were difficulties in finding it. It was detected in 18 - 33% of cases.
Upper first molar.
The palatal and distal roots usually contain a type I canal. In Caucasians, the length of this tooth is about 22 mm, the palatal root is slightly longer than the cheek roots. In the teeth of Mongoloids, there is a tendency for the roots to be closer and denser, and the average tooth length is slightly shorter.
The pulp chamber is quadrangular in shape and wider in the bucco-palatal direction than in the mediodistal direction. It has four pulp horns, of which the mediobuccal one is the longest and sharpest in outline, and the distal buccal horn is smaller than the mediobuccal horn, but larger than the two palatine ones. The bottom of the pulp chamber is usually located below the level of the neck and is rounded with a convexity towards the occlusal surface. The mouths of the main canals are funnel-shaped and lie in the center of the roots. The lesser mediobuccal canal, if present, lies on the line connecting the orifices of the mediobuccal and palatine canals. If this line is divided into three parts, then the mouth of the additional canal will lie about the first third, closer to the medial buccal main canal.
It must be remembered that the shape of the incisions in the neck area and at the level of the middle of the crown of the pulp chamber are of different configurations (the shape of the incision in the neck area is more diamond-shaped than quadrangular). In this regard, the mouth of the mesiobuccal canal is closer to the buccal wall than the mouth of the distal canal is to the distal wall. Therefore, the distal buccal root, and therefore the mouth of its canal, is closer to the middle of the tooth than the distal wall of the chamber. The mouth of the palatine canal is usually easy to find.
There is considerable variation across cross sections. The mesiobuccal canals are usually the most difficult to instrument because they run in a medial direction. The lesser medial buccal canal is often very narrow and tortuous and connects to the main canal. Since both medial buccal canals lie in the buccopalatal plane, they often overlap each other on the radiograph. Additional difficulties are encountered due to the frequent curvature of the mesiobuccal root in the distal direction in the apical third of the root.
The distobuccal canal is the shortest and often narrowest of the three canals and extends distally from the chamber, being oval in shape before becoming round towards the apex. Typically the canal curves medially in the apical half of the root.
The palatine canal is the largest and longest of all three main canals and has a round cross-section along its entire length, tapering towards the apex.
About 50% of the palatine roots are not straight, but curve towards the buccal side in the apical part (4-5 mm from the apex). This curvature is not visible on the x-ray.
With age, the canals become narrower and their mouths are more difficult to find. Secondary dentin is deposited mainly on the roof of the pulp chamber and, to a lesser extent, on the floor and walls. Due to this, the pulp chamber becomes very narrow between the roof and the bottom. This can lead to furcation perforation, especially when using a turbine handpiece, if the operator does not notice the narrow chamber. To prevent this complication, it is advisable to limit the use of a turbine handpiece to the preparation of enamel and, partially, dentin, and to complete the formation of access at low speeds. You can estimate the distance between the bump and the roof of the chamber on the radiograph. This distance is marked on the forest and serves as a guide.
Relatively recent clinical observations highlight variations in the anatomy of the dental canals of these teeth. There are reports of teeth with two palatal canals.
Misconception
Since a tooth consists of roots and a pre-crown part, there is sometimes a misconception that there are as many canals in teeth as there are roots . This is far from true, because the canals quite often branch and bifurcate near the pulp. Moreover, several channels can run parallel to each other in one root. There are also cases of their bifurcation at the apex, which means that one root has two apices and this, of course, complicates the work of doctors when filling such teeth.
Taking into account all the features of the individual structure of teeth, dentists need to be very careful when treating and filling, so as not to miss any branch. After all, sometimes without an x-ray it is very difficult, even during an autopsy, to identify how many canals there are in the teeth.
The development of modern medicine and dentistry in particular, today makes it possible to increasingly preserve those diseased teeth that just yesterday had to be removed due to the impossibility of treatment. The procedure for treating root canals in teeth is itself quite complex, because they are filled with soft tissue - pulp, which contains a large number of nerve endings, blood vessels and other connective tissues. Today, this is dealt with by a separate branch of dentistry – endodontics, the development of which makes it possible to improve the condition of a person’s teeth and cure even complex problems in more than 80% of cases, preserving the tooth itself.
The goals of this treatment are:
- Removing developing infection inside the root system;
- Preventing pulp decay or removing it;
- Removal of infected dentin;
- Preparing the canal for filling (giving it the desired shape);
- Increasing the effect of medications.
The difficulty of such treatment of the root system is that it is quite difficult for the dentist to get to the diseased canals and control the progress of the procedure. After all, if you do not remove even a microscopic part of the infection, it can develop again over time.
One of the main indicators for such treatment is the inflammatory process, which leads to damage to the soft tissue of the pulp inside the canals. Most often, various diseases such as caries and pulpitis lead to this, but root canal treatment may also be necessary for periodontitis.
The first symptoms of the need for such treatment are tooth pain or swollen gums. However, it is worth considering that if the disease passes into the chronic stage, pain may not be observed, but the disease develops and will ultimately lead to tooth loss. This is why it is so important to have regular dental checkups.
Upper second molar
Upper second molar.
Usually this tooth is a small replica of the first molar, but the roots usually diverge less and the fusion of the two roots is more common. The predominant form is with three canals and three apical openings, the average length is 21 mm.
Fusion of roots is found in 45-55% of Caucasians, and Mongoloids in 65 to 85% of cases. In these cases, usually the mouths of the canals and they themselves are located closer to each other or merge.
Access contours in the upper molar.
Lower central and lateral incisors
Lower first incisor. (I channel configuration type).
Both teeth have an average length of 21 mm, although the central incisor is slightly shorter than the lateral incisor. The morphology of dental canals can have one of three configurations.
Lower second incisor. (IV channel configuration type).
Type I - one main canal from the pulp chamber to the apical foramen.
Type II/III - two main canals that merge in the middle or apical third into one canal with one apical foramen.
Type IV - the two main canals remain separate for the entire length of the root and with two apical foramina.
All studies show that type I is the most predominant. Two channels are recorded in 41.4% of cases, and type IV - in 5.5% of cases.
There is evidence that in Mongoloids, two canals are less common in these teeth.
The pulp chamber is a small replica of the upper incisors. There are three pulp horns, not very well defined, and the chamber is wider in the labial-lingual direction. In the version with one channel, it can bend towards the distal and, less commonly, towards the labial side. The canal begins to narrow in the middle third of the root and becomes round. With age, the changes are the same as in the upper incisors and the pulp chamber can be located below the level of the neck of the tooth.
Specifics of treatment of three-channel pulpitis
Treatment of pulpitis of a 3-canal tooth is considered complex and must be carried out with special care. In severe cases, several visits to the dentist are required.
- The doctor spends an hour to an hour and a half on a multi-channel tooth;
- under a microscope - about two hours.
This is due to the fact that 3-channel pulpitis requires treatment in each process.
Treatment under a microscope
Treatment of three-channel pulpitis is carried out by a specialist in the field of endodontics. Work in the dental canals is best done under a dental microscope. This method has many advantages.
Advantages of treatment under magnification
- The dental canals are very thin, tortuous, no more than 1 mm in diameter. The microscope magnifies them to 2.5-3 cm. The dentist does not treat blindly, under magnification he clearly sees all the branches and foci of inflammation. Treatment of pulpitis of the 3rd canal takes place in good lighting.
- The patient lies down, the doctor looks not into the mouth, but into the microscope camera. This has a calming effect on dentophobes.
- The microscope reveals the most difficult to reach areas for the doctor. This is especially true for patients who have hidden dental canals that are not visible to the human eye. And during endodontic treatment, it is important to remove all foci of inflammation to avoid relapse.
Lower canine
Lower canine. (I channel configuration type). (By Harty).
This tooth resembles the upper canine, although its size is smaller. Very rarely it has two roots. Its average length is 22.5 mm. Type I canal is the most prevalent, but the main deviation in canines is the variant with two canals (frequency about 14%). In less than 6% of cases, a type IV canal configuration with two separate apical foramina is found.
Access to lower incisors and canines
Essentially, the approach is identical to that in the upper teeth. However, with a pronounced curvature towards the lingual side of the crowns of the incisors and due to very thin (especially in older people) canals, it is sometimes necessary to involve the cutting edge and, sometimes, the labial surface of the tooth into access to avoid bending of the instrument.
The outlines of the access in the lower canine are shown in Fig.
Access contours in the lower incisors.
Access contours in the lower canine.
Lower premolars
These teeth usually have a single root, but sometimes the first premolar may have a bifurcated root in the apical half.
Type I channel predominates. Where there are two canals (usually in the first premolar), there may be type IV/V configurations. Types II/III occur in less than 5% of cases. The highest incidence of two canals is reported to be 10.8% in the second premolar (Zillich and Dowson, 1973).
One report found that two canals in the first premolar were three times more common in African-Americans than in whites (Trope et al., 1986). This option is more common among southern Chinese. In less than 2%, three canals may be present in the first premolar.
The pulp chamber of the lower premolars is wider in the buccolingual direction than in the mesiodistal direction, and has two horns, the buccal one being better developed. The lingual horn is small in the first premolar and larger in the second premolar.
Lower first premolar. (II channel configuration type). (By Harty).
The canals of the lower premolars are similar to the canines of the canine, although they are smaller, but they are also wider in the bucco-lingual direction until the middle third of the root, when they narrow and acquire either a rounded shape or bifurcate.
Lower second premolar. (I channel configuration type). (By Harty).
Lower first molar
Typically this tooth has two roots, a mesial and a distal. The latter is smaller and usually rounder than the medial one. Among Mongoloids, there is a variant with an additional distal-lingual root with a frequency of 6 to 43.6% (Walker, 1988).
Lower first molar. (By Harty).
This double-rooted tooth usually has three canals, the average length of the tooth is 21 mm. Two canals are located in the medial root. In 40 - 45% of cases, there is only one apical foramen in the medial root. The single distal canal is usually larger and more oval than the medial canals, and in 60% of cases opens on the distal surface of the root, close to the anatomical apex.
The attention of specialists was attracted by the work of Skidmore and Bjorndal (1971), who showed that in the distal canal there are two canals in more than 25% of cases. In Mongoloids, due to the tendency to double the distal root, the frequency of occurrence of two canals in this root is even higher - about half (Walker, 1988).
There have been reports of cases involving five channels.
Lower first molar with five canals. (By Harty).
The pulp chamber is wider at the medial than at the distal wall and has five pulp horns. The lingual horns are taller and pointed. The bottom is rounded with a convexity towards the chewing surface and lies immediately below the level of the cervix. The mouths of the canals are funnel-shaped, and the medial canals are narrower than the distal ones.
Of the two medial canals, mediobuccal and mediolingual, the first listed is the most difficult to pass due to its tortuosity. It leaves the pulp chamber in a medial direction, which changes to a distal direction in the middle third of the root. The mesiolingual canal is slightly wider and usually straight, although it may curve medially in the apical third of the root. These two canals can have a dense network of anastomoses among themselves along their entire length.
When an additional distal canal is present, it is more lingual and tends to curve toward the buccal side.
With age, dentin deposition occurs on the roof side, and the canals narrow.
How many canals in teeth: table and location diagram, anatomy and functions
Despite their different shapes, human teeth are structured the same.
Each has a neck, crown and root, hidden in the alveolus - a special depression in the jaw. Each root is connected to the jaw by connective tissue; its space is filled with nerve fibers, blood vessels, and collagen.
The correct treatment and restoration of each dental unit largely depends on the number and placement of root canals.
Tooth root: structure, length, purpose
The root of each tooth is located in its own alveolar cavity, hidden by the gum. It (like a tooth) consists of dentin, covered on the outside with cement - bone tissue that comes into contact with the enamel next to the dental neck. The entire structure, together with the connective fibers, forms a shell between the alveolus and cement (periodontium).
Depending on the location, the root can be single or branched. Normally, the maximum number of root cavities is 4. Their length depends on the size of the tooth; it necessarily reaches the bundle of vessels and nerves of the alveoli, from where the unit receives nutrients. It is determined using an apexlorator probe, which is immersed in the hole until it jams.
The function of the root is to secure the tooth in the gum, for which a strong ligamentous apparatus is provided. Its channels provide access to the nerves, arteries and veins to the coronal part. Thanks to this, the tooth receives nutrition, develops, and is sensitive to external influences. Due to innervation, the tooth is a full-fledged organ located in the oral cavity.
Why do we need a channel in the first place?
A canal is an anatomical space within a tooth root. They act as a continuation of the pulp chambers, each of which represents a single tooth cavity and duplicates the contours of dental crowns in shape.
Healthy canals contain nerves and blood vessels that are responsible for metabolism.
Each canal begins as an orifice at the neck of the tooth and ends with an apical foramen at a distance from the central apex of the root.
After removal of the nerves (in case of complicated caries, infection), the canal openings are filled with special pins and fillers. Teeth deprived of nutrition darken.
How many canals are there in each tooth?
The number of dental canals and nerves is determined by the doctor. Their number does not always correspond to the number of roots of a dental unit. The dentist can determine the exact amount using an x-ray (see.
See also: what is the name of a photograph of all teeth and how is it taken?). On average, there are from 1 to 3 of them, 4 are less common. The upper “eights” (wisdom teeth) can have 5 canals, which makes their removal extremely difficult.
The “eights” of the lower jaw contain no more than 3 cavities.
Root canals are distinguished by structure and divided into different types:
- I. They have a simple anatomy, starting at the base of the pulp chamber and going to the apex of the root. Therapy is not difficult.
- II. Two canals that have a common origin at the bottom of the pulp chamber and merge into one at the apical foramen.
- III. At the base of the pulp capsule, a wide orifice opens, from which one passage emerges. In the lower third of the root, it is divided into two paths, which connect at its base and end in a common exit.
- IV. Two independent canals of simple anatomical shape, each with its own apical foramen.
- V. One canal is located inside one root. Near the top it is divided into two independent entrances. It can be difficult for the dentist to treat them to the apical foramen.
- VI. 2 canals extend from the bottom of the pulp, merge into one at the base and diverge again, opening with separate apical openings.
- VII. The root canal originates from the bottom of the pulp chamber, narrows at the middle of the root, distributing into two cavities that connect at the apex, and again branch into two separate ones (resembling the shape of a chain link).
- VIII. There are three independent direct channels in one root. From a morphological point of view, their structure is very simple, but the frequency of distribution is low.
- IX. The three root cavities of the tooth diverge and merge at the base into one with a single morphological exit. This anatomy is found in third molars.
Upper jaw: incisors, canines, premolars and molars
Lateral, additional branches can depart from the main ones at any level and have a simple and rather complex configuration.
Important indicators and characteristics are shown in the table:
| Upper jaw tooth | Length of dental unit/canal, mm | Number of roots/number of channels | Features taken into account by dentists during extirpation and treatment |
| Central incisors | 23/13 | 1/1 | |
| Lateral incisors | 22/12,9 | 1/1 |
|
| Fangs | 27/15,9 | 1/1 |
|
| First premolar | 21/13,6 | 2 (80%)/2 (95%), less common with 1 or 3 canals, root |
|
| Second premolar | 22/14,4 | 1 (90%)/1 (75%), there are cases when teeth have two canals, two and three roots |
|
| First molar | 21/13,3 | 3/3, in 40% of cases there are four-channel teeth, in 15% - 2 roots |
|
| Second molar | 20/13 | 3 (80%)/3 (57%), there is a high probability that the teeth will have 4 cavities (40%), less common are units with 1, 2 roots and the same number of passages |
|
Lower jaw: incisors, canines, premolars and molars
The teeth of the lower and upper jaws are called the same, but have some differences in structure, as can be seen in the photo. The farther they are located, the more channels they find. The topographical features of the dental units of the lower jaw, information about how many roots there are in them, are given in the following diagram of the anatomy of the root canals:
| Lower jaw tooth | Length of a dental unit, mm | Number of roots/number of channels | Features taken into account by dentists during extirpation and treatment |
| Incisors | 21–22/13 | 1/1, in 40% of cases there are 2 channels. |
|
| Fangs | 26/15,3 | 1/1 In 2% of cases, two-rooted teeth, 2 canals are observed |
|
| First premolar | 22/13,7 | 1/1, in 20% of cases there may be two cavities in the teeth, in 5% - three |
|
| Second premolar | 22/15,2 | 1/1, 10% – 2 channels |
|
| First molar | 21/14,5 | 2/3, 13% – two channels, 7% – four |
|
| Second molar | 20/14,1 | 2/3, in 13% two canals are found, in 7% four-canal teeth are found |
|
Possible norm options
Accurate information about the number of cavities in the sixth, seventh and other human teeth cannot be found anywhere. This is due to the individuality of the structure, partly genetic disposition.
Dentists rely on average statistical data and use x-rays if necessary. The orthopanogram shows the teeth of the upper and lower jaws.
Sight images provide information about a specific root tooth that is being examined.
An x-ray will show how many canals are in the premolar tooth from above. It is he who is exposed to the main chewing load. The quadruples or first premolars of the maxilla usually have two root branches.
The fives following them also have two channels, despite the heavy load they have to absorb. 3 roots are considered a normal variant, but this happens only in 6% of clinical cases.
Mandibular premolars with three canals are not observed. Normally there is one branch, in 20% of cases there are two.
Large fourth and fifth molars have a large number of canals. The top sixes can have three or four of them with equal probability. The same picture is observed in the lower jaw.
The top sevens, as in the photo, usually have 3-4 branches, the bottom ones - 2 or 3.
Since the posterior molars are almost the same in structure, the doctor can tell with almost 100 percent probability how many canals the patient has in them.
Topography indicates that a person normally has from 1 to 4 dental canals. However, there may be nuances that are unexpected for the doctor and the patient. The maximum number of canals that dentists observe is six. Each of them is subject to complex endodontic treatment. Without it, it is impossible to save the tooth.
READ ALSO: How is dental canal cleaning done?
How to find out how many canals there are in a tooth, and what is it for?
Knowledge of the topography of the tooth cavity is important for correct endodontic treatment. During depulpation, the canal cavity is cleaned, the main passage is formed and hermetically sealed. At the same time, a barrier is restored that prevents the penetration of carious infection and bacteria into the bloodstream.
In ordinary life, the patient does not need to know how many roots and canals he has in his tooth. However, if the units are destroyed or hurt, an x-ray will be taken when visiting a doctor. It will show the degree of tissue damage, the number and length of the dental canals, their branches and structural features.
If narrow and long canals are detected, a computed tomography scan can be performed, which helps to accurately determine the configuration. In addition to the number and length of the canals, which is determined instrumentally, the doctor needs information about their patency:
- with a curvature of up to 25 degrees, they are considered instrumentally accessible;
- curvature within 25–50 degrees can be difficult to pass;
- a change in direction over 50 degrees is inaccessible for instrumental intervention; if the angle is located near the mouth, specialists can try to improve patency.
It happens that the doctor does not find the canal at all, which is due to its narrowing or overgrowing as a result of a long-term inflammatory process. Another reason why cavities are difficult to detect is age-related changes and incorrect dental treatment in the past.
The complex anatomy of the canals causes difficulties in their treatment. The instrument entry cavity may be curved. It may contain pathogenic microorganisms that are resistant to traditional antiseptic drugs.
A highly qualified dentist can overcome these problems and provide high-quality root canal treatment for complicated caries, pulpitis and periodontitis.
His arsenal includes the necessary diagnostic equipment that will show how many roots are present in the tooth, and tools for canal treatment.
Source: https://AzbukaZubov.com/stomatolog/o-zubax/skolko-kanalov-v-zubah-tablitsa.html
Lower second molar
In Caucasians, the second molar resembles a small version of the first, with an average length of 20 mm. There are two canals in the medial root, and only one in the distal root. The medial canals tend to merge in the apical third and form a single apical foramen.
Lower second molar. (By Harty).
Studies conducted in 1988 showed a high tendency for root fusion in the Chinese (33-52% of cases). In a longitudinal section, such teeth resemble a horseshoe. Where there is incomplete root separation, incomplete canal separation may occur, which is accompanied by a dense network of anastomoses between the canals and can lead to unpredictable localization of the orifices. One of the locations was called the middle buccal orifice with the middle buccal canal. In Caucasians, this anomaly is recorded in 8% of cases, which is significantly less than in the Chinese.
How much will treatment cost in Moscow clinics?
Treatment of pulpitis of a three-channel tooth will cost the patient a lot. The price in Moscow dentistry starts from 5,000 (without a filling on the crown) - 7,000 rubles (with the simplest filling) and reaches 13,000 rubles. Treatment under a microscope increases the cost of 3-channel pulpitis to 21,000 rubles. The prices for treatment of pulpitis are influenced by the quality of the instruments used by the doctor, the choice of anesthesia, means for disinfecting the canals, as well as the material from which the filling is made. All this needs to be taken into account before going to the doctor.
Lower third molar
This tooth is often underdeveloped with numerous and poorly developed cusps. Usually there can be as many canals as there are cusps. The root canals are relatively larger than those of other molars, possibly due to the late development of this tooth.
Despite these disadvantages, it is usually less difficult to fill the roots of a lower than an upper wisdom tooth because access is usually easier due to the mesial inclination of the tooth and because they more often follow normal anatomy, resembling a second molar, and are less likely to be deviated from the norm.
Why is it important to treat baby teeth?
Now that it is clear that the structure of baby teeth is very similar to permanent teeth, the question “To treat them or not to treat them” should not arise for parents at all. Advanced caries often leads to destruction and damage to the pulp. Then the roots become involved in the pathological process. Removing dental nerves is not a pleasant procedure. It is important to prevent its occurrence.
Moreover, refusal of dental treatment can result in a number of other problems. This means:
- Incorrect bite formation. If, due to the destruction of the crown, the doctor has to remove it ahead of time, voids appear in the row, which “neighbors” tend to occupy. Then, by the time the “adult” unit erupts, there may not be a place for it - it will begin to grow somewhere on the side and ruin the smile.
- Damage to future teeth even before they erupt. With deep caries and periodontitis, cysts often form. They affect the rudiments of permanent teeth. Then the child is faced with the fact that his new tooth turns out to be sick and requires urgent treatment. Needless to say, its service life will be significantly reduced because of this.
- Diseases of the gastrointestinal tract. If parents believe that it is better to remove baby teeth rather than treat them, then by the age of nine their child (especially if he is prone to developing dental diseases) may lose half of his teeth. Is it possible to fully chew food in such a situation? No. The child regularly swallows poorly chewed foods. Because of this, the load on the intestines increases, which can result in frequent abdominal pain, stool disorders, nausea, gastritis and more serious gastrointestinal diseases.
- Psychological complexes. At 9-10 years old, a child evaluates his appearance and sees that his smile is very different from the smiles of his peers - it does not have a large number of teeth or they are dark in color, half destroyed. Because of this, he begins to be embarrassed to smile, laugh, and tries to talk less. All this negatively affects his self-esteem and does not allow him to quickly adapt to new situations and successfully go through the process of socialization in elementary school.
Don't waste your children's teeth. Teach your child from childhood to undergo preventive examinations in the pediatric dentistry department. At the same time, choose a specialist for him who you can trust. Then the child will not perceive another visit to the dentist as something terrible. He will be happy to go to the appointment, knowing that he will not be hurt.
Access in lower molars
Access contours in lower molars.
If there is a second distal canal in the first molar, a more quadrangular approach may be necessary. Care must be taken when removing the roof of the pulp chamber to avoid damaging the bottom. To improve visual control of the canal mouths, access can be expanded. The access walls should extend toward the occlusal surface to resist masticatory forces and prevent displacement of temporary fillings.
If the course of the channels is non-standard, access can be expanded and/or modified.
Thus, standard, universal, tabular methods for determining the working length of dental canals cannot currently satisfy clinicians. Of course, you need to have a more or less correct idea about possible deviations in the morphological characteristics of cavities; the decisive factor is an X-ray examination with the introduction of files into the root canal. In this case, it is advisable not to try to insert the instrument to its full working length, since it is almost impossible to obtain undistorted radiographs.
What diseases cause inflammation of dental canals?
Root canals can become inflamed due to the development of the following diseases:
- caries;
- pulpitis;
- periodontitis.
An accurate diagnosis of inflammation of the pulp and canals of the tooth can only be determined by a dentist after X-ray diagnostics and a visual examination of the oral cavity.