Molars are divided into canines, incisors, premolars, and molars. The first three types of teeth erupt in place of similar milk teeth. In turn, molars do not have predecessors and appear behind the temporary ones, therefore their second name is accessory.
Each jaw has 16 teeth - four incisors, two canines, four premolars and six molars. In some cases, third molars, better known as wisdom teeth, do not erupt because they do not have buds in the jaw - then instead of 16, a person has 14 teeth above and below. Experts explain this phenomenon by a reduction, or simplification, of the dental system caused by changes in dietary style.
Anatomical features of the upper teeth
- The central incisor (the largest of all eight) has a chisel-shaped crown with a convex surface and one cone-shaped root. The only root canal in 75% of cases is straight.
- The lateral incisor with the same chisel-shaped crown and the same convex surface has a characteristic depression in the enamel - a “blind fossa”. There is one root canal, but more often it is deviated to the side.
- The canines on the upper dentition are often larger than those on the bottom. They are characterized by a crown pointed on all sides and the longest cone-shaped root. Canines have a single root canal, which can be straight (45%), distally deviated (30%) or vestibular deviated (12%).
- The first premolar with a prism-like crown is characterized by a convex lingual surface. On the chewing side there are tubercles, and between them there is a fissure. In the upper dentition, these teeth are always larger than in the lower one. The root has extended longitudinal grooves, which divide it in 60% of cases into two parts - buccal and palatal. There are often also two root canals.
- The second premolar with the same prism-shaped crown has predominantly one straight cone-shaped root with expanded lateral surfaces. Sometimes the root bifurcates closer to the top. There are often two root canals.
- The first molar is the largest tooth in the dentition. The rectangular crown has a diamond-shaped chewing surface with four cusps and an H-shaped fissure between them. There are usually three root canals, but sometimes there are 4 (25%) or 5 (1%).
- The second molar with a classic cube-shaped crown has 4 cusps and an X-like fissure on the chewing side. The tooth has 3 roots and three (87%) or four (13%) canals.
What is an apex locator used for?
Back in 1965, Seltzer and Bender showed that the quality of endodontic treatment depends on three mandatory components - thorough cleaning of the canal, sterilization and its complete obturation. The basis of successful endodontic treatment is the correct determination of the working length of the root canal. If this stage of treatment is neglected, it becomes impossible to carry out all subsequent stages in a high-quality manner, and as a result, the quality of the entire endodontic treatment is significantly reduced.
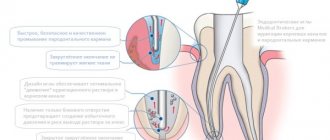
The working length of the root canal is the distance between the external landmark on the tooth crown and the apical border. In the anatomy of the apex, three structures are important: the apex proper (radiographic apex), the large apical foramen, and the apical constriction. The apical constriction zone is recommended as the physiological apical level for instrumentation and root canal filling.
The apical constriction is the area of the apical part of the root canal with the smallest diameter (Ricucci & Langeland 1998). Microscopic and morphometric studies of root canals have shown that, as a rule, the apical narrowing does not coincide with the dentino-cemental boundary, as previously thought. From the apical constriction to the large apical foramen, a funnel-shaped expansion of the root canal occurs, which is not possible to carefully treat. According to a number of authors, in 75% of cases the apical foramen is deviated from the main axis of the tooth. This means that the radiographically determined apex and apical constriction are often located at different levels, so serious inaccuracies can arise when using radiographs alone to determine the working length of the root canal.
There are several methods for determining the working length of the root canal: tabular, tactile, radiological, red dot (paper point) method, patient reaction, electronic (using apex locators).
According to statistics, during the initial passage of the root canal, the dentist can tactilely determine the apical constriction in 75% of cases. When treating non-vital teeth, one can additionally be guided by the patient’s reaction to the advancement of the instrument in the root canal. When reaching the apical foramen, the patient feels a slight prick.
One of the popular methods for determining working length is x-ray. In this case, control radiographs are taken at the stage of endodontic treatment with the instrument inserted and during the process of filling the root canal. However, the position of the apical constriction varies significantly and may change depending on the patient’s age, parafunction of the masticatory muscles, apical resorption and other factors. According to histomorphometric measurements carried out by Dummer et al. (1984), the average distance between the apical constriction and the anatomical tip is 0.51 mm. In more than 92% of cases, the apical narrowing is 0.5 mm from the anatomical and 1.0 mm from the radiographic apex.
Based on the anatomy of the apex, researchers recommend root canal treatment 0.5-2 mm from the radiographic apex of the root, because the zone of apical constriction is in this range with the highest statistical probability. The radiograph is a two-dimensional image and does not reproduce the entire anatomy of the apical part of the root; layering and distortion of the image are often noted. Chunnetal. (1981) found that 43% of the files found at the apex on radiographs were actually located behind the apex (in the periodontium). When interpreting radiographic data, a potential error is the subjectivity of the investigator. Therefore, it is not advisable to be guided only by this method of determining the working length.
During the process of drying the root canal, blood on a paper point can also help determine the working length (red dot method). Blood on the tip of the paper point indicates excessive expansion of the apical foramen and extension of the instrument beyond the apex. The size of the blood spot corresponds to the length by which the working length of the canal should be reduced. This method is also not objective and depends on the characteristics of the clinical situation.
The apex location method is based on the constancy of electrical resistance of tissues. Since the hard tissues of the tooth have a higher resistance than the mucous membrane of the oral cavity and periodontal tissue, the electrical circuit between the electrodes placed on the lip and in the canal remains open until the file reaches the periodontal tissue. Apex locators of the first generations worked only in a dry and clean channel and determined the strength of direct current. Starting from the third generation, apex locators determine impedance using alternating currents of different frequencies (starting from 5 frequencies of apex locators of the 3rd generation, to dual-frequency apex locators of the 5th generation). The impedance is lowest in the region of apical constriction and greatest in the region of the greater apical foramen. Thus, all modern apex locators measure precisely this point of drop in resistance. Therefore, no apex locator can measure the length of the root canal, we cannot get a metric result even if the apex locator has a millimeter scale.
The fifth generation apex locators include Raypex 5 (VDW). Raypex 5 features digital impedance measurement technology, clear LCD color display and improved measurement accuracy. The device runs on battery power.
The lip electrode is attached to the lip opposite the tooth being examined. The root canal should be moist, but excess fluid in the tooth cavity is undesirable. The doctor can observe the progress of the file on the device display. Once the file reaches the apical third of the canal, an enlarged image of the apex appears on the screen indicating the position of the file in relation to the apical foramen.
Raypex 5 display start
A graphical representation of the position of the instrument apex is accompanied by a sound signal of varying intensity depending on its approach to the apex. In the image of the apical third of the canal, several segments of different colors are highlighted: green indicates the zone of apical constriction, yellow indicates the large apical foramen, red indicates the instrument extends beyond the apex, and a continuous sound signal is heard. As a rule, for vital teeth, it is recommended to treat the root canal to the green zone. In the case of non-vital teeth and periodontitis, it is recommended to treat the root canal to the yellow area. Thus, an enlarged image of the apical part of the root canal with graduated sections allows the dentist to decide at what level to complete the canal treatment. In addition, the dentist can independently set the so-called “virtual apex” - a point in the apical zone, upon reaching which the frequency of apex locator sound signals will sharply increase.
An additional advantage of working with the Raypex 5 apex locator is the presence of a demo mode, which allows you to quickly master working with it, as well as explain the principle of operation to the patient. In addition, the convenient folding body allows for easy viewing of the display from any angle.
The undoubted advantage of measuring the root canal using an apex locator is that it is significantly more accurate than that using radiography. Studies evaluating apex locators have shown an accuracy of determining the working length within 0.5 mm of the apical foramen in 75-93.4% of cases.
Errors in determining the working length of the root canal using an apex locator can be associated with contact of electrodes with metal structures in the oral cavity, the presence of perforation, a broken instrument, an open apex or apical resorption, the presence of a large amount of liquid in the tooth cavity, as well as when the battery charge is less than 50 %.
Examination of the length of the root canal with an apex locator in combination with x-ray examination is the most complete. You cannot completely trust only one method for determining working length. It is advisable to combine several methods at once.
Author: Maria Kamenskikh, dentist, road dental clinic, Yekaterinburg
Where and how is it better to buy an apex locator?
The purchase of any modern dental equipment is always associated with serious financial costs and risks. Today it is not enough to find the right model; the main task is to carefully check the supplier’s company through all possible channels. It is necessary to involve in this work not only a doctor who will determine the necessary functionality of the equipment, but also an accountant and a lawyer. All this entails additional costs. Is it possible to do without them?
The Dentists Club marketplace is rightfully considered one of the most reliable and positively proven resources. This aggregator has been successfully operating in the dental market since 2021 and has already proven itself as a trusted and honest partner. At the same time, the Dentist Club market is the only aggregator of offers in the field of dentistry today, which allows you not only to purchase the necessary goods at the guaranteed best prices, but also in addition to receive a 1.5% cashback back to your account!
What other benefits does the Dentist Club market provide?
1. Time saving
- You don’t need to go to all the search results sites to find what you need
- There is no need to call companies and try to explain to them over the phone what you need
- No need to send a request and wait for managers of trading companies to answer or call you back
2. The Dentist Club Market service helps when communicating with doctors
- You can easily find the desired product by description and photo
- Determine the desired model and its modification
- Check all these parameters directly with your doctor and get his approval
- Place an order in one click.
3. Lowest prices on the market guaranteed
- You can simultaneously see the prices of all companies offering the required product
- Compare the prices presented and choose the most profitable one
- The manager of the selected company will call you back. He doesn’t need to explain ten times what you need, because... He sees all the necessary information in the generated order.
- And don't forget about cashback!
4. 100% order security
- Absolutely all companies - suppliers of dental equipment and consumables, collaborating with the marketplace, have already been checked for legal purity by lawyers of the Dentists Club. That is why all purchases made on the Dentists Club market are absolutely reliable!
5. Ease of use
- You can install the Dentist Club Market service on your phone so that it is always at hand. Open the app, find the products you need, and order. Everything is quick, accessible and simple. Application in the App Store on iPhone (iOS) or on Google Play for Android.
Go to Market >>>
Anatomical features of the lower teeth
- The central incisor is the smallest tooth in the “adult” bite and the smallest among the incisors. The root is quite short, in 65% of cases there is one root canal, less often - two.
- The chisel-shaped lateral incisor is always larger than the central one. One or less often two root canals – both narrow. “Adult” incisors on the lower jaw are less susceptible to damage than others, so dentists rarely turn to them for the treatment of caries in children and adults.
- Fang - similar in structure to the upper one, but is smaller in size. In 96% of cases it has a single root canal of normal structure.
- The first premolar has a rounded crown in cross-section and two characteristic tubercles on the chewing side. One root is slightly flattened.
- The second premolar is very similar in crown shape to the canine, and is always larger than the adjacent premolar. The surfaces of the single root are smooth and slightly shiny. Two roots occur in only 3% of cases or less.
- The first molar with a cubic crown has five cusps on top of the crown, separated by an F-like fissure. In 88% of cases, three root canals are formed.
- The second molar is smaller than the first, but completely replicates its anatomical features. Root canals are curved and have poor patency. In 85% of cases, the tooth has three canals, in 10% - four.
The anatomical characteristics of teeth are similar in all people, but each person may have individual characteristics, for example, the absence of wisdom teeth or an increased number of root canals in a particular tooth.