Treatment of diseases of the oral mucosa caused by herpes infection in children.
Currently, the most common viral infection in childhood is herpetic, which is explained not only by the widespread prevalence of the herpes simplex virus, but also by the peculiarities of the formation of the immune system in the developing child’s body.
One third of the world's population is affected by herpes infection and more than half of these patients suffer several attacks of infections per year, often including manifestations in the oral cavity.
It has been established that the infection rate of children with the herpes simplex virus between the ages of 6 months and 5 years is 60%, and by the age of 15 it is 90%. A similar problem is typical for pediatric dentistry, since the incidence of acute (primary) herpetic stomatitis in children increases every year.
The role of the herpes simplex virus in diseases of the oral mucosa was first pointed out at the beginning of the twentieth century. N.F. Filatov (1902). He suggested the possible herpetic nature of the most common stomatitis in children - acute aphthous. This evidence was obtained later when antigens of the herpes simplex virus began to be detected in the epithelial cells of the affected areas of the oral mucosa.
According to the International Statistical Classification of Diseases and Related Health Problems, latest tenth revision (ICD-10, Geneva, 1995), this disease is classified as acute herpetic stomatitis (AHS). Acute herpetic stomatitis not only ranks first among all lesions of the oral mucosa, but is also included in the leading group among all infectious pathologies of childhood. Moreover, in every 7-10th child, acute herpetic stomatitis very early turns into a chronic form with fairly frequent relapses
EPIDEMIOLOGY AND PATHOGENESIS.
The herpes simplex virus is very widespread in nature. It causes various diseases of the central and peripheral nervous system, liver, other parenchymal organs, eyes, skin, mucous membrane of the gastrointestinal tract, genital organs, and also has a certain significance in the intrauterine pathology of the fetus. Often in the clinic there is a combination of various clinical forms of herpetic infection. Acute herpetic stomatitis is characterized by high contagiousness among non-immune people.
The widespread occurrence of the disease between the ages of 6 months and 3 years is explained by the fact that at this age, antibodies received from the mother through the placenta disappear in children and there are no mature specific immune systems. Among older children, the incidence is significantly lower due to acquired immunity after herpetic infection in its various clinical forms.
In the development of herpes infection, which manifests itself mainly in the oral cavity, the structure of the oral mucosa in children of different ages and the activity of local tissue immunity are of great importance. The highest prevalence of acute herpetic stomatitis in the period up to 3 years may be due to age-morphological characteristics, manifested by high permeability of histohematic barriers during this period and a low level of cellular immune reactions due to the thinness of the epithelial cover with low levels of glycogen and nucleic acids, friability and weakness of differentiation of the basement membrane and fibrous structures of connective tissue (abundant vascularization, high levels of mast cells with their low functional activity, etc.).
The pathogenesis of acute herpetic stomatitis has not been sufficiently studied at present. In all cases, viral infection begins with the adsorption of viral particles and penetration of the virus into the cell. Further ways of spreading the introduced virus throughout the body are complex and little studied. There is some evidence of the spread of the virus by hematogenous and neural routes. During the acute period of stomatitis in children, viremia occurs.
The lymph nodes and elements of the reticuloendothelial system are of great importance in the pathogenesis of the disease, which is quite consistent with the pathogenesis of the sequential development of clinical signs of stomatitis. The appearance of lesions on the oral mucosa is preceded by lymphadenitis of varying severity. In moderate and severe clinical forms, bilateral inflammation of the submandibular lymph nodes often develops, but all groups of cervical lymph nodes can be involved in the process. Lymphadenitis in acute herpetic stomatitis precedes eruptions of lesions in the oral cavity, accompanies the entire course of the disease and remains for 7-10 days after complete epithelialization of the elements.
Both specific and nonspecific immune defense factors play a role in the body’s resistance to the disease and in its protective reactions. Studies of nonspecific immunological reactivity in AGS have revealed violations of the body's protective barriers, reflecting the severity of the disease and periods of its development. Moderate and severe forms of stomatitis led to a sharp suppression of natural immunity, which was restored 7-14 days after the child’s clinical recovery.
CLINICAL PICTURE.
Acute herpetic stomatitis, like many other infectious diseases, occurs in mild, moderate and severe forms. The development of the disease goes through five periods: incubation, prodromal, period of disease development, extinction and clinical recovery. During the development of the disease, 2 phases can be distinguished - catarrhal and rash of lesions.
During this period, symptoms of damage to the oral mucosa appear. Initially, intense hyperemia of the entire oral mucosa appears, and after a day, less often two, elements of the lesion are usually found in the oral cavity. The severity of acute herpetic stomatitis is assessed by the severity of the manifestations of toxicosis and the nature of the damage to the oral mucosa.
The mild form of acute herpetic stomatitis is characterized by an external absence of symptoms of intoxication of the body; the prodromal period is not clinically manifested (see figure).
Figure 1. - Herpetic stomatitis, mild form.
The disease begins suddenly with an increase in temperature to 37-37.5°C. The general condition of the child is quite satisfactory. Sometimes minor inflammation of the nasal mucosa and upper respiratory tract is detected in the oral cavity. Also in the oral cavity, symptoms of hyperemia and slight swelling occur, mainly in the area of the gingival margin (catarrhal gingivitis). The duration of the period is 1-2 days. The vesicle stage is usually reviewed by parents and the doctor, because. the bubble quickly bursts and turns into aphthae. Afta is a round or oval-shaped erosion with smooth edges and a smooth bottom with a rim of hyperemia around it.
In most cases, against the background of increased hyperemia, single or grouped lesions appear in the oral cavity, the number of which usually does not exceed 6. Single rashes. The duration of the disease development is 1-2 days. The period of extinction of the disease is longer. Within 1-2 days, the elements acquire a marble-like color, their edges and center are blurred. They are already less painful. After epithelialization of the elements, the phenomena of catarrhal gingivitis persist for 2-3 days, especially in the area of the anterior teeth of the upper and lower jaw. In children suffering from this form of the disease, as a rule, there are no changes in the blood, sometimes only towards the end of the disease a slight lymphocytosis appears. In this form of the disease, the protective mechanisms of saliva are well expressed: pH 7.4 ± 0.04, which corresponds to the optimal state. During the height of the disease, the antiviral factor interferon appears in saliva (from 8 to 12 units/ml). The decrease in lysozyme in saliva is not pronounced.
Natural immunity in a mild form of stomatitis suffers slightly, and during the period of clinical recovery, the child’s body’s defenses are almost at the level of healthy children, that is, in a mild form of acute herpetic stomatitis, clinical recovery means the complete restoration of the impaired defenses of the body.
The moderate form of acute herpetic stomatitis is characterized by fairly clearly defined symptoms of toxicosis and damage to the oral mucosa during all periods of the disease. Already in the prodromal period, the child’s well-being worsens, weakness, moodiness, loss of appetite appear, and there may be catarrhal tonsillitis or symptoms of an acute respiratory infection. The submandibular lymph nodes enlarge and become painful. The temperature rises to 37-37.5°C.
As the disease progresses during the development of the disease (catarrhal phase), the temperature reaches 38-39°C, headache, nausea, and pale skin appear. At the peak of the rise in temperature, increased hyperemia and severe swelling of the mucous membrane, elements of the lesion appear, both in the oral cavity and often on the skin of the face in the perioral area. There are usually from 10 to 25 lesions in the oral cavity. During this period, salivation increases, saliva becomes viscous and viscous. There is pronounced inflammation and bleeding of the gums. Rashes often recur, which is why when examining the oral cavity one can see elements of the lesion that are at different stages of clinical and cytological development. After the first eruption of lesions, body temperature usually drops to 37-37.5°C. However, subsequent rashes are usually accompanied by a rise in temperature to the previous levels. The child does not eat, sleeps poorly, and symptoms of secondary toxicosis increase.
An ESR of up to 20 mm/h is observed in the blood, often leukopenia, sometimes slight leukocytosis. Band leukocytes and monocytes are within the upper limits of normal, lymphocytosis and plasmacytosis are also noted. An increase in the titer of herpetic complement-fixing antibodies is detected more often than after suffering a mild form of stomatitis.
The duration of the period of extinction of the disease depends on the resistance of the child’s body, the presence of carious and damaged teeth, and the rationality of therapy. Under unfavorable conditions, the elements of the lesion merge, their subsequent ulceration, and the appearance of ulcerative gingivitis. Epithelization of the lesion elements takes up to 4-5 days. Gingivitis, severe bleeding and lymphadenitis last the longest.
With a moderate course of the disease, the pH of saliva becomes more acidic, reaching 6.96 ± 0.07 during rashes. The amount of interferon is lower than in children with a mild course of the disease, does not exceed 8 units/ml and is not found in all children. The content of lysozyme in saliva decreases more than in mild forms of stomatitis. The temperature of the externally unchanged oral mucosa corresponds to the child’s body temperature, while the temperature of the lesion elements in the degeneration stage is 1.0-1.2° lower than the temperature of the unchanged mucous membrane. With the beginning of regeneration and during the period of epithelization, the temperature of the affected elements increases by approximately 1.8° and remains at a higher level until complete epithelization of the affected mucous membrane.
The severe form of acute herpetic stomatitis is much less common than the moderate and mild form. During the prodromal period, the child has all the signs of an incipient acute infectious disease: apathy, adynamia, headache, musculocutaneous hyperesthesia and arthralgia, etc. Symptoms of damage to the cardiovascular system are often observed: bradycardia and tachycardia, muffled heart sounds, arterial hypotension . Some children experience nosebleeds, nausea, vomiting, and pronounced lymphadenitis of not only the submandibular, but also the cervical lymph nodes.
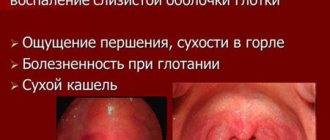
During the development of the disease, the temperature rises to 39-40°C. The child develops a mournful expression on his lips and painful, sunken eyes. There may be a mild runny nose, coughing, and somewhat swollen and hyperemic conjunctivae of the eyes. Lips are dry, bright, parched. In the oral cavity, the mucous membrane is swollen, clearly hyperemic, with pronounced gingivitis.
After 1-2 days, up to 20-25 lesions begin to appear in the oral cavity. Often, rashes in the form of typical herpetic blisters appear on the skin of the perioral area, eyelids, conjunctiva of the eyes, earlobes, and on the fingers like a panaritium. Rashes in the oral cavity recur, so at the height of the disease in a seriously ill child there are about 100 of them. The elements merge, forming large areas of mucosal necrosis. Not only the lips, cheeks, tongue, soft and hard palate are affected, but also the gingival margin. Catarrhal gingivitis turns into ulcerative-necrotic. There is a sharp putrid odor from the mouth, profuse salivation mixed with blood. Inflammation in the mucous membranes of the nose, respiratory tract, and eyes worsens. Streaks of blood are also found in secretions from the nose and larynx, and sometimes nosebleeds are observed. In this condition, children need active treatment from a pediatrician and dentist, and therefore it is advisable to hospitalize the child in the isolation ward of a pediatric or infectious diseases hospital.
In the blood of children with severe stomatitis, leukopenia, a band shift to the left, eosinophilia, single plasma cells, and young forms of neutrophils are detected. In the latter, toxic granularity is very rarely observed. During the period of convalescence, as a rule, herpetic complement-fixing antibodies are detected.
An acidic environment is noted in saliva (pH 6.55 ± 0.2), which can then be replaced by a more pronounced alkaline reaction (8.1-8.4). Interferon is usually absent, the content of lysozyme is sharply reduced.
The period of extinction of the disease depends on the timely and correct administration of treatment and on the child’s history of concomitant diseases.
Despite clinical recovery, a patient with a severe form of acute herpetic stomatitis experiences profound changes in homeostasis during the period of convalescence.
DIAGNOSTICS.
The diagnosis of acute herpetic stomatitis is made based on the clinical picture of the disease. The use of virological and serological diagnostic methods in practical healthcare is difficult. This is due, first of all, to the complexity of special research methods. In addition, with these methods, results can be obtained, at best, towards the end of the disease or some time after recovery. Such a retrospective diagnosis cannot satisfy the clinician.
In recent years, the immunofluorescence method has found wide application in medicine. The high percentage of agreement (79.0 ± 0.6%) in the diagnosis of acute herpetic stomatitis based on immunofluorescence data and the results of virological and serological studies makes this method the leading one in diagnosing the disease. The essence of the immunofluorescence method is to detect the specific luminescence of squamous epithelial cells obtained from lesions by scraping and stained with fluorescent antiherpetic serum. The ability to obtain an answer within 2.5-3 hours from the moment of sampling makes the method of etiological express diagnosis of stomatitis very promising. The percentage of positive results increases if the material for immunofluorescence research is obtained in the first days of the eruption of lesions in the oral cavity.
TREATMENT.
The treatment tactics for patients with acute herpetic stomatitis should be determined by the severity of the disease and the period of its development. Complex therapy for acute herpetic stomatitis includes general and local treatment. For moderate and severe disease, it is advisable to carry out general treatment together with a pediatrician.
Due to the peculiarities of the clinical course of acute herpetic stomatitis, rational nutrition and proper organization of feeding the patient occupy an important place in the complex of therapeutic measures. Food must be complete, i.e. contain all the necessary nutrients and vitamins. Therefore, it is necessary to include fresh vegetables, fruits, berries, and juices in your diet. Before feeding, it is necessary to anesthetize the oral mucosa with a 2-5% anesthesin solution or lidochlorgel.
The child is fed predominantly liquid or semi-liquid food that does not irritate the inflamed mucous membrane. Great care must be taken to ensure adequate fluid intake. This is especially important during intoxication. During meals, natural gastric juice or its substitutes should be given, since pain in the oral cavity reflexively reduces the enzymatic activity of the stomach glands.
During the prodromal period, the following is used: interferon - 3-4 drops in the nose and under the tongue every 4 hours.
Local treatment.
Local therapy for acute herpetic stomatitis has the following objectives:
- relieve or reduce painful symptoms in the oral cavity;
- prevent repeated rashes of lesions (reinfection);
- promote the acceleration of epithelization of lesion elements.
From the first day of the development of acute herpetic stomatitis, taking into account the etiology of the disease, local antiviral therapy should occupy an important place. For this purpose, it is recommended to use 25% oxolinic, 0.5% tebrofen, 0.5% bonaftone, interferon ointments, and acyclovir ointment. It is recommended to use these medications repeatedly (3-4 times a day) not only when visiting a dentist, but also at home. influence both the affected areas of the mucosa and the area without pathological changes, since they have a greater preventive effect than a therapeutic one.
Painkillers before meals:
- 5-10% solution of anesthesin in peach oil;
- lidochlor gel.
Means for treating the oral cavity after each meal:
- potassium permanganate solution 1:5000;
- furatsilin solution 1:5000;
- a strong solution of freshly brewed tea;
- solutions of enzymes - trypsin or chymotrypsin.
During the period of rashes, antiviral drugs (Florenal, Tebrofen, Bonafton, acyclovir) are prescribed in combination with bacterial lysates. They are applied to the oral mucosa after its hygienic treatment 3-4 times a day. The preparation of a mixture of bacterial lysates is prescribed up to 8 tablets per day. Solutions of neoferon and interferon are also used.
During the period of extinction of the disease, keratoplasty agents are used - rosehip oil, carotoline, sea buckthorn oil, in combination with a mixture of bacterial lysates.
It should be noted that AGS in any form is an acute infectious disease and requires in all cases the attention of a pediatrician and dentist in order to provide comprehensive treatment, eliminate contact of a sick child with healthy children, and carry out preventive measures in children's groups.
V.M. Elizarova, S.Yu. Strakhova, E.E. Kolodinskaya,
Moscow State Medical and Dental University,
Scientific Center for Children's Health, Russian Academy of Medical Sciences, Moscow
published 02/08/2012 20:43 updated 08/22/2016 — Dentistry
Products for the prevention and hygiene of children's oral cavity
The most common means are toothpaste and brush. A children's brush has soft and delicate bristles and a small head, as well as a small, comfortable handle and often has an original and beautiful shape. The toothpaste has a pleasant taste, due to which the baby is not discouraged from the procedure in the initial stages of growing up.
Oral wipes are another effective hygiene product because they contain xylitol, which inhibits the growth of dangerous bacteria that can cause tooth decay. Such napkins are indispensable when teeth are just emerging and cannot be cleaned with a toothbrush.
Dental floss is a hygiene product that allows you not only to remove food debris stuck between your teeth, but also to promptly remove plaque.