Algorithm for restoration of the coronal part of the upper molars in a therapeutic dentistry clinic
Over the past decades, we have witnessed a significant introduction of the latest technologies and materials available on the global dental market into the therapeutic dentistry clinic. Achieving a high-quality final result when implementing any type of dental therapy is possible only if a harmonious combination of shape, color and functional characteristics of the restorations is ensured.
Restoration of missing tissues must be carried out as close as possible to the natural anatomical features of the individual’s dentofacial apparatus. The correctness of the restored forms is the leading link in restoration technology. The process of competent modeling of the anatomical shapes of teeth leads to the fact that the newly formed structures made of composite materials are harmoniously combined with the environment of the oral cavity. The subsequent condition and functioning of the entire dental system depends on how the final restoration of hard dental tissues is carried out.
When restoring damaged dental tissues, dentists, first of all, need to use knowledge of anatomy, morphometry, and odontoglyphics. The anatomical features of the upper molar are demonstrated (Fig. 1).
| 1 - mediovestibular tubercle or paracone. 2 - distovestibular tubercle or metacone. 3 -mediopalatal tubercle or protocone. 4 -distopalatinal tubercle or hypocopus. 5 - Karabel tubercle. 6 - additional distal tubercle. 7 - vestibular groove. 8 - medial groove. 9 - central groove. 10 - distopalatinal groove. 11 - distal fossa. |
Rice. 1. Anatomical features of the upper molar
Most often, the coronal part of the upper molars has a cube- or diamond-shaped shape and, as a rule, consists of four main cusps:
- mediovestibular (1) or paracone,
- distovestibular (2) or metacone,
- mediopalatal (3) or protoconus
- distopalatinal (4) or hypocopus (Fig. 1).
The additional tubercle of Karabel (5) is located on the lateral surface of the mediopalatal tubercle (protocone).
Conditionally uniting with each other, the mediovestibular, mediopalatal and distovestibular form a trigon (triangle), and the distopalatinal occupies the talon (heel). An additional distal tubercle (6) is located between the distovestibular tubercle (2) (metaconus) and the distopalatinal tubercle (4) (hypocopus).
All tubercles are separated from each other by first-order grooves:
- vestibular groove (7), separates the anterior and posterior buccal cusps,
- medial groove (8), separates the anterior buccal and anterior palatal cusps, c
- central groove (9), separates the main tubercles,
- distopalatinal groove (10), separating the distopalatinal tubercle from the main tubercles.
Before proceeding with the restoration of missing dental tissues, it is necessary to establish their belonging to a certain functionally oriented group and determine the number and color of the cusps.
There are different anatomical forms of the upper molars: four-cusp (1,2,3,4), which in turn are divided into teeth with crushing of the distopalatinal (5.5a) and distovestibular (6.6a) cusps, three-cusp (7.8) and two-cusp (9) teeth (Fig. 2).
Rice. 2. Varieties of shapes of the crown part of human upper molars
We present to your attention a series of drawings that show the stages of restoration of the coronal part of the upper molar using modular technologies in aesthetic dentistry (Lomiashvili 2004).
During an objective examination, the crown part of the 16th tooth was destroyed by 1/2 (Fig. 3). However, despite the rather voluminous defect of hard tissues, the crown of the upper first molar has a cube-shaped shape, consisting of four main cusps directed towards the fissure of the first order, H-shaped.
| A – vestibular side; B – palatal side; C – medial side; D – distal side. |
Rice. 3. Crown of the 16th tooth before the preparation stage
The coronal part of the 16th tooth after the preparation stage is demonstrated (Fig. 4).
| A – vestibular side; B – palatal side; C – medial side; D – distal side. |
Rice. 4. Crown of the 16th tooth after the preparation stage
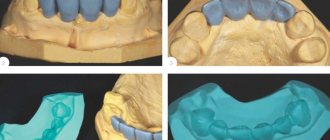
To restore the coronal part of a tooth, filling materials of any curing method can be used (photopolymers, chemically curing materials, glass ionomer cements). Light-curing materials from DMG EcuSphere ® were used in the study.
The imitation of “dentine mass” is made with a material with a darker shade (Fig. 5). Imitation of “enamel mass” with the same material with a lighter shade (Fig. 6).
| Rice. 5. Imitation of “dentin mass” | Rice. 6. Imitation of “enamel mass” |
Rice. 5, 6 . A – vestibular side; B – lingual side; C – medial side; D – distal side
On the existing surface, specified by certain dimensions - length (medio-distal parameter), width (vestibular-palatal parameter) of the tooth crown (Fig. 7) - we presumably outline the location zones of the main 4 cusps.
| A – vestibular side; B – palatal side; C – medial side; D – distal side. |
Rice. 7. Crown of the 16th tooth restored with filling material
Using minor depressions in the form of a fissure of the first order, we distinguish a trigon (triangle), consisting of the mediopalatal, mediovestibular and distovestibular tubercles, and a talon (heel), which occupies the distopalatinal tubercle, while we form the buccal tubercles slightly higher than the palatine ones (Fig. 8). These actions are performed using tools with a special coating for working with composite materials.
| 1 - mediovestibular tubercle, 2 - distovestibular tubercle, 3 - mediopalatal tubercle, 4 - distopalatinal tubercle. A – vestibular side; B – palatal side; C – medial side; D – distal side. |
Rice. 8. Isolation of trigon (triangle), coupon (heel)
We begin shaping the surfaces of the teeth using burs from the KIT “CARBIDE Trimming & Finishing Bur” kit (Fig. 9). Bur No. 1 is ovoid (9406). Needle-shaped bur No. 2 (9903). Bur No. 3 form CFT 1. Bur No. 4, CFT 3 form.
| Bur No. 1 ovoid shape (9406). Bur No. 2 needle-shaped (9903). Boron No. 3 form CFT1. Boron No. 4 form CFT3. |
Rice. 9. “SS White t” burs. KIT “CARBIDE Trimming & Finishing Bur”
Using an ovoid-shaped bur No. 1 (9406), we contour the projections of the main cusps, forming first-order grooves, determining their locations on the occlusal surface of the crowns of the 16th tooth (Fig. 10, 11).
Rice. 10, 11. Formation with bur No. 1 of an ovoid shape (9406) of the projection of the main tubercles ( A – vestibular side; B – palatal side; C – medial side; D – distal side.)
Next, we use needle-shaped bur No. 2 (9903). The shape of this bur is more elegant compared to the shape of bur No. 1, which allows it to penetrate into deeper layers of the filling mass and leave a thinner mark on the surface. We also use this bur to separate the main tubercles of the chewing surface from each other, forming the vestibular, medial and distopalatinal grooves of the first order (Fig. 12, 13).
Rice. 12, 13. Formation of needle-shaped grooves (9903) with a bur No. 2 of the first order ( A – vestibular side; B – palatal side; C – medial side; D – distal side)
Thus, the formation of the main morphological elements of the occlusal surface, consisting of mediopalatal, mediovestibular, distovestibular and distopalatinal cusps, has been completed.
Using bur No. 3 of the CFT 1 form, we identify second-order grooves within each tubercle, which leads to the identification of the main morphological elements within this surface: the main longitudinal (1), medial (2) and distal (3) ridges (Fig. 14).
| 1 - main longitudinal ridge, 2 - medial ridge, 3 - distal ridge. A – vestibular side; B – palatal side; C – medial side; D – distal side. |
Rice. 14. Using bur No. 3 of the CFT1 form, we select furrows of the second order, which leads to the selection of: the main longitudinal ( 1 ), medial ( 2 ) and distal ( 3 ) ridges
We also form triangular pits, due to which a clearer differentiation of the chewing surface is achieved (Fig. 15).
| A – vestibular side; B – palatal side; C – medial side; D – distal side. |
Rice. 15. Using bur No. 3 of CFT1 form, we form triangular pits
Thanks to microrelief modeling, the external shape and volume of the restored object is gradually recreated. Next, it is necessary to isolate the individual components of this morphological unit inside each main cusp on the chewing surface of the 16th tooth.
As the chewing surface of the 16th tooth is formed, not only the geometric shapes of the burs change, but also the number of their faces. At the initial stages of forming the chewing surface, we use burs with 12 edges, then we move on to burs with 30 edges.
The need to use both 12 and 30-sided burs is explained, first of all, by the cutting properties of the burs. Thus, 12-sided burs effortlessly remove excess composite from the surface of restorations, determining the final dimensions and shape. 30-sided burs complete the process by polishing the surface, removing only minor irregularities.
We consider it necessary to note that a perfectly smooth and glossy surface is achieved by using only 30-sided burs. Therefore, we recommend that restorations be pre-treated with 12-sided carbide burs and final polished with 30-sided carbide burs.
Using a bur (No. 4) of form CFT 3, we shape the transition from the chewing surface to the side surfaces by smoothing out the protruding shapes (Fig. 16).
| A – vestibular side; B – palatal side; C – medial side; D – distal side. |
Rice. 16. Formation by bur (No. 4) of the CFT3 shape of the transition from the chewing surface to the lateral surfaces
One of the important elements of modeling a tooth crown is the formation of first-order (palatal and vestibular) grooves on the lateral surfaces (Fig. 17).
| A – vestibular side; B – palatal side; C – medial side; D – distal side. |
Rice. 17. Formation of CFT3-shaped grooves of the first order on the lateral surfaces with a bur (No. 4)
When using these burs, there is no need for a grinding stage, because We used 30 grain burs in the last stages. Due to the fact that the burs have twice as many edges as the burs used in the first stage, they remove even less tissue in one rotation, due to which the effect of a smooth surface is achieved (Fig. 18).
| A – vestibular side; B – palatal side; C – medial side; D – distal side. |
Rice. 18. Crown of the 16th tooth before the polishing stage
After completing the main stages of building the microrelief of the chewing surface, it is necessary to achieve a smoother shape of the tooth crown; this can be done using silicone polishing heads and circular brushes with polishing paste.
In conclusion, a series of drawings of the restored coronal part of the 16th tooth from the chewing, vestibular, palatal and two contact surfaces is demonstrated (Fig. 19-24).
| Rice. 19. Chewing surface | Rice. 20. Vestibular surface |
| Rice. 21. Palatal surface | Rice. 22. Medial surface |
| Rice. 23. Distal surface | Rice. 24. Distal surface (modular technologies) |
Rice. 19-24. A – vestibular side; B – palatal side; C – medial side; D – distal side
A clinical example of restoration of the coronal parts of teeth 16 and 17 is demonstrated (Fig. 25-36).
| Rice. 25. Initial clinical situation, the patient is 20 years old. Teeth 16 and 17 were previously treated for caries. There are fillings that do not match the color and shape of the natural tissues of the tooth crowns. The shrinkage of the fillings and an incorrectly formed contact point in the area of the 16th tooth are also determined. | Rice. 26. 16, 17 teeth after the stage of preparation and removal of dental plaque. |
| Rice. 27. 16, 17 Imitation of “dentine mass” | Rice. 28. 16, 17 Imitation of “enamel mass” |
Shaping tooth surfaces with burs. From the KIT "CARBIDE Trimming & Finishing Bur".
| Rice. 29. Formation by bur No. 1 of an ovoid shape (9406) of the projection of the main tubercles. | Rice. 30. Formation of needle-shaped grooves (9903) with bur No. 2 of the first order. |
| Rice. 31. Using bur No. 3 of the CFT1 form, we select furrows of the second order, which leads to the selection of: the main longitudinal (1), medial (2) and distal (3) ridges. | Rice. 32. Using bur No. 3, form CFT1, we form triangular pits. |
| Rice. 33. Formation by bur (No. 4) of the CFT3 shape of the transition from the chewing surface to the lateral surfaces. | Rice. 34. Formation of CFT3-shaped grooves of the first order on the lateral surfaces with a bur (No. 4). |
To give a more natural shine, you need to perform a polishing step.
Rice. 35, 36. The final result of treatment of 16, 17 teeth using modular technologies in aesthetic dentistry (Lomiashvili L.M., 2004).
In conclusion, the authors of the article recommend that dentists adhere to this algorithm for constructing occlusal forms of molar crowns. The use of these technologies will reduce the working time for restoring missing dental tissues, and will also give calm, confidence and clarity to medical procedures, ensuring a decent final result that is close to natural forms.
Modern methods.
Methods for restoring teeth are determined depending on the condition of the dental system, so in some cases one or another method is prescribed. In any case, modern dentists try to preserve living tissue and restore the tooth whenever possible, and prosthetics are prescribed only as a last resort. Dental restoration using prosthetics allows you to avoid further disturbances in the dental system. Failure of at least one component of the dental system has a significant impact on the functioning of the system, so prosthetics help maintain function and prevent possible failures. Tooth restoration, in addition to restoring the patient’s chewing function, is also a prevention of dysfunction of the masticatory muscles and TMJ.
It is necessary to understand that prosthetics is the best way to restore a tooth in cases of complete loss. Modern technologies make it possible to restore a lost tooth as carefully as possible to healthy tissues, observing all aesthetic and anatomical standards. Dental prosthetics are performed using removable or fixed structures, depending on the clinical situation, the individual characteristics of the patient and his preferences. Removable dental prosthetics require periodic replacement of removable structures; fixed dentures are installed taking into account long-term wear.
Causes of destruction
The dental organs are daily under the influence of stress when chewing food, they are exposed to an acidic environment, and are attacked by various bacteria. Due to these factors, teeth deteriorate, even if they are thoroughly cleaned daily. Most people, as a result, experience caries or other diseases that destroy enamel and dentin.
In addition, causes of destruction include:
- Hidden caries, the cavity of which is not visible, since it is hidden, and unnoticed erosion of the tooth occurs.
- Sharp weight loss.
- A diet when the body does not receive the necessary elements.
- Time of bearing and feeding a child.
- Diseases of the gastrointestinal tract and urinary system, metabolic disorders.
- Impacts, accidents, falls, etc.
- Frequent exposure of the teeth to too cold or hot food, as well as drinks.
- Removal of the nerve, after which the tooth can easily collapse.
- The influence of aggressive chemical components, including those contained in some mouth rinses and toothpastes.
- Endocrine diseases, chemotherapy and radiation therapy.
Use of composite materials
Restoring a dental organ after its destruction using composite materials is simple and inexpensive. However, this method cannot always be applied. It is used only if no more than 30 percent of the dental crown is destroyed. Otherwise, the filling will quickly fall out.
Building up a tooth with a composite involves expanding the cavity, cleaning it of damaged tissue and forming a crown with a composite. In this case, the doctor determines the condition of the dental nerve. If it is damaged, it is removed. Sometimes, in order to test the tooth, a temporary filling is placed on it, which will make it possible to understand whether the pulp will cause concern to the patient.
To build up the front incisors and canines, a light composite is often used, which has the property of refracting light in much the same way as tooth enamel. For this reason, it will not be noticeable among living teeth. The material is very durable and non-toxic. You can choose the most suitable shade. Another advantage of its use is that hardening occurs only from ultraviolet rays, so the doctor can slowly form the crown, giving it the desired shape, repeating the shape of a living dental organ.
Price
We offer an overview of turnkey prices in Moscow clinics for prosthetics:
| Clinic | Address | Price |
| Dentistry Good Crocodile | St. Perovskaya, 16 | From 1800 rub. |
| Dentistry IceDent | St. 10th Parkovaya, 3 | From 3200 rub. |
| Dento Dento-El | St. Sadovaya-Samotechnaya, 13 | From 2700 rub. |
| Dentistry Magic Smile | St. Tvardovskogo, 12 | From 4600 rub. |