The selective grinding technique is used for periodontal diseases. The procedure is performed to eliminate increased pressure on diseased tissues. Grinding teeth improves nutrition and blood circulation in the periodontium. There are several options for carrying out the technique, but they all have one goal - to eliminate unfavorable factors that interfere with the restoration of diseased tissues.
Indications
Selective tooth grinding is a complex procedure that requires a strictly individual approach to each patient. In some cases, achieving an ideal ratio is impossible due to the structure of the jaw and individual teeth. In this case, the procedure is carried out in order to get as close as possible to the desired result.
The main purpose of grinding is to create uniform contact throughout the entire dentition, remove excessive load on the jaw and distribute it evenly over all teeth. To do this, hard tissues are ground off from the teeth that come into contact during chewing movements, after which they are aligned with the dentition, on which there are no points of contact.
Main indications for the procedure:
- improper closure of molars;
- increased tone of the masticatory muscles;
- displacement or deformation of the dentition due to injury;
- lack of natural tooth wear;
- abnormalities in the structure of the jaw;
- prevention of periodontal diseases.
In some cases, the grinding method is used to grind down sharp edges of teeth, which injure the tongue and oral mucosa. This saves the patient from minor injuries or damage.
Main directions
All grinding techniques are based on two main directions.
The basic methods include Jenkelson and Schuyler methods:
- Selective grinding according to the Jenkelson method - occlusal relationships are made in a convenient form by the patient himself without the doctor’s efforts. Premature contacts are removed directly in the central/distal occlusion, while anterior/lateral adjustments cannot be made.
- Schuyler method - with this correction method, occlusal contacts are subject to correction, which created interference with the articulation of the rows. They are removed in the following sequence: first distal/central, then anterior, and lastly lateral occlusion. The specialist manually regulates the movement and position of the jaw.
According to Jenkelson, there are 3 classes of unwanted contacts, according to which the procedure is carried out.
The surfaces of the slopes of the mounds are marked with the symbols I, II, III, the surfaces of the antagonists - I a, II a, III a:
- I – vestibular
slopes of the cervical tubercles of the lower 6-8 teeth, 4-5 teeth, the surface of the anterior ones, facing the vestibule of the oral cavity; - I a – oral slopes of the cervical tubercles of the upper 6-8 teeth, 4-5 teeth, the surface of the anterior ones, which faces the vestibule of the oral cavity;
- II – oral slopes of the upper palatine cusps of 6-8 teeth, 4-5 teeth;
- II a – vestibular slopes of the lower 6-8 teeth, 4-5 teeth (lingual cusps);
- III – vestibular slopes of the upper 6-8 teeth, 4-5 teeth (palatal cusps);
- III a – oral slopes of the lower 6-8 teeth, 4-5 teeth (buccal cusps).
Contraindications
Sanding is not carried out in the following cases:
- During the period of progressive periodontal inflammation. In this case, before the main procedure, the patient is prescribed a course of treatment.
- The patient has been diagnosed with dental anomalies and deformations that require treatment by other specialists (orthopedist or surgeon).
- Acute and chronic diseases of the temporomandibular joint are observed.
The grinding procedure should only be carried out by a qualified specialist. Incorrectly performed correction can lead to displacement of teeth, excessive load on the periodontium due to flattening of the dental tubercle, and removal of one or more teeth from occlusal contact.
How does the procedure work?
The operation is carried out in several stages, with short breaks.
Preparation for the procedure is based on a preliminary visual examination of the patient. Closing the dentition helps to identify points of contact between the dental surface and the arch where this closure is absent. Next, final (more accurate) testing is done using carbon paper to identify all problem areas for further occlusion correction.
Based on the data obtained, zones for grinding are selected. The procedure itself may seem unpleasant, so it is usually carried out under the influence of an anesthetic. A preliminary test for allergic reactions eliminates all negative consequences from the use of painkillers.
The grinding procedure is carried out in three stages:
- At the first stage, a preliminary grinding procedure is carried out in order to eliminate the most pronounced unevenness of the dental surfaces. In case of significant shortening of teeth, mandatory depulpation is carried out.
- Next, the procedure is carried out on other teeth that require correction.
- After final polishing, fluoride-containing polishing pastes are used.
After each stage, treatment is carried out with special preparations that reduce tooth sensitivity.
In case of periodontal diseases, grinding is performed to eliminate premature occlusal contacts, which lead to horizontal traumatic overload of the teeth. The possibility of overload increases with periodontitis due to disruption of the physiological process of abrasion of hard dental tissues. The preserved unworn cusps of premolars and molars, as well as the cutting edges of the incisors, cause premature contacts in central, anterior and lateral occlusions. The periodontium of these teeth experiences load in the mesial, distal, vestibular (labial or buccal side) and oral (lingual or palatal side) directions.
In case of periodontal diseases, grinding is performed to eliminate premature occlusal contacts, which lead to horizontal traumatic overload of the teeth. The possibility of overload increases with periodontitis due to disruption of the physiological process of abrasion of hard dental tissues. The preserved unworn cusps of premolars and molars, as well as the cutting edges of the incisors, cause premature contacts in central, anterior and lateral occlusions. The periodontium of these teeth experiences load in the mesial, distal, vestibular (labial or buccal side) and oral (lingual or palatal side) directions. With each closure of the dentition, the teeth deviate in the corresponding direction, causing compression of the periodontium and disruption of its trophism, increasing the resorption of bone tissue from the overloaded walls of the alveoli. In addition, premature contacts can lead to parafunctional conditions, which are accompanied by dysfunction of the masticatory and facial muscles and temporomandibular joints.
According to the method proposed by V. A. Jankelson (1979), premature contacts that appear only with central occlusion are eliminated. Lateral and anterior articulatory movements of the lower jaw are not corrected using this technique.
Jenkelson's technique is called the functional method. During the grinding process, the doctor does not control or correct the movements of the lower jaw.
According to Jenkelson’s classification, premature contacts are divided into three classes: class I includes contacts on the vestibular slopes of the buccal cusps of molars and premolars and the vestibular surface of the lower incisors, class II includes contacts on the oral slopes of the palatal cusps of the upper molars and premolars, class III includes contacts on the vestibular slopes of the palatal cusps of the upper molars and premolars.
Premature contacts of classes I and II lead to a displacement of the lower jaw to the lateral side, and the corresponding teeth experience functional overload directed to the oral or vestibular side. Class III contacts promote displacement of the mandible to a mesial eccentric position.
By selective grinding of premature contacts of classes I and II, horizontal overload of the teeth is eliminated. In addition, some narrowing of the chewing surface of the teeth helps to reduce the occlusal load on the periodontium. In this case, parafunctional lateral displacements of the lower jaw are eliminated.
Grinding the mesial slopes of the cusps of molars and premolars prevents sagittal shift of the mandible. During the grinding process, a decrease in the height of the bite is unacceptable.
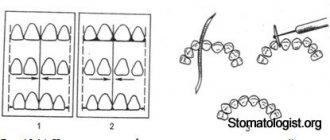
Selective grinding of teeth is best done in strict sequence. You should start by grinding down premature contacts in the central occlusion. They are easily identified using occludograms. To eliminate diagnostic errors when obtaining occludograms, the patient is asked to tightly close the lateral teeth on both sides several times. Then a wax plate is applied to the lower dentition and the patient is asked to independently (without the help of a doctor) close the dentition in the position of central occlusion. The places pressed on the plate through the resulting holes are projected onto the teeth using a soft pencil, after which the wax is removed.
Selective grinding of class I premature contacts from the vestibular surfaces of the buccal buds of molars and premolars is carried out by rounding the abrasion facets along their periphery and slightly sharpening the tubercles of these teeth. If it is necessary to grind a significant amount, the oral slopes of the buccal cusps of the upper molars and premolars can be partially grinded (class 1a). This prevents the occurrence of increased sensitivity of the enamel and dentin of the lower teeth.
After eliminating premature contacts in the area of the lateral segments (right and left) of the lower dentition, you can begin to correct the contacts of the anterior teeth in central occlusion. In this case, it is necessary to grind the vestibular surfaces of the lower incisors and canines, eliminate premature contacts and partially reduce the width of the worn cutting edge. Grinding should be continued until control occludograms show thinning of the wax plate only at the tops of the cusps of molars and premolars and along the cutting edge of the incisors.
To identify premature contacts of class II, wax plates are applied to the dentition of the upper jaw in the lateral sections. Depressed areas are marked on the teeth with a soft pencil. Peripheral areas are corrected along the edge of the occlusal facets of premature contacts. During the process of selective grinding, shortening of the palatal cusps of the upper lateral teeth is unacceptable. After proper grinding, the peripheral edges of the occlusal facets should be smoothed and rounded, and the palatal cusps of these teeth should be slightly sharpened, so that closure with antagonists is carried out freely, without any obstacles. Grinding is continued until only the tops of the palatine tubercles leave marks in the wax on the control occludograms.
A very important place in selective grinding of teeth in central occlusion is occupied by the elimination of class III supracontacts according to Jenkelson. They are located on the vestibular slopes of the palatal cusps of the upper molars and premolars. To identify them, a wax plate is placed on the upper lateral teeth. When the dentitions close in the areas of supracontacts, the wax is pressed through (perforated).
Premature contacts of class III are eliminated by flattening the vestibular slopes of the palatal cusps of the upper molars and premolars. If significant grinding is necessary, the corresponding antagonist areas are prepared, i.e., the oral slopes of the buccal cusps of the lower molars and premolars. These slopes are called Sha class supra-contacts.
When selectively grinding such contacts, you need to be very careful. Excessive grinding of the palatal cusps of the teeth of the upper jaw and the buccal cusps of their antagonists should not be allowed, as they maintain the height of the bite (interalveolar height). During the grinding process, a decrease in the height of the bite is unacceptable.
After correctly performed selective grinding of teeth in central occlusion, simultaneous bilateral multiple occlusal contact of the dentition of the upper and lower jaws is restored. Patients do not feel any difference in the closure of the dentition on the right and left. On the control occludograms, the traces of the areas of the teeth that maintain the height of the central occlusion are expressed equally. Elimination of premature contacts in distal occlusion and during excursion of the lower jaw from distal to central occlusion. Distal occlusion is characterized by multiple simultaneous contacts of the teeth of the upper and lower jaws. In this case, the lower jaw occupies a posterior (retrusive) position, which is designated by the Latin letters RKP (retrocuspid position).
To accurately identify premature contacts, it is best to use a diagnostic occludogram. If there is no standard wax blank for obtaining an occludogram, then you need to take two strips of wax (preferably clasp wax) measuring 3x4 cm, slightly heat it up and squeeze the molars and premolars of the upper jaw on the left and then on the right with your fingers. These teeth are first dried. The lower exposed surface of the wax is moistened with water to prevent sticking to the teeth of the lower jaw.
Then you can begin distal displacement of the mandible. To achieve this goal, the doctor places the palm of his right hand on the chin, places the index and thumb of the left hand on the chewing surface of the lower molars and premolars and asks the patient to calmly, without tension, close the dentition. The patient tries to move his jaw back so as not to bite the doctor’s fingers. At this time, the doctor uses his right hand to apply light pressure on the chin, as a result of which the lower jaw is directed to the dietal (retrusive) position, thereby achieving distal occlusion. These measures are well known to orthopedists, as they are widely used in determining and fixing the mesiodistal relationship of the jaws in cases of complete loss of teeth.
To obtain distal occlusion, you can also ask the patient to raise the tip of the tongue upward and backward and reach the mucous membrane of the soft palate or swallow saliva.
When the dentitions close in areas of premature contact, the wax is pressed through (perforated). Most often, supracontacts are found on the mesial slopes of the palatal cusps of the molars and premolars of the upper jaw. These areas are marked (marked) on the teeth with a soft pencil and the wax is removed.
Due to the fact that sometimes it is necessary to grind off tissue not only from the upper, but also from the lower molars and premolars, it is necessary to identify contacts on both jaws. To do this, strips of wax are applied in the same way to the lower lateral teeth on both sides. Using the same techniques, the maximum posterior displacement of the lower jaw is achieved and distal occlusion is obtained. Areas of depressed (perforated) wax are marked on the teeth with a pencil, the wax is removed and selective grinding of the teeth begins.
In case of distal occlusion, premature contacts should be eliminated on the mesial slopes of the vestibular slopes of the palatal cusps of the upper molars and premolars and the distal slopes of the oral slopes of the buccal cusps of the lower molars and premolars (III and Ilia classes, according to Jenkelson), since it is in these areas that premature contacts are most often observed . In abbreviated form, this rule is denoted in the dental literature by the Latin letters MODU (Medial, Ober, Distal, Unter), which means mesial upper, distal lower.
You should start by eliminating premature contacts on the lateral teeth of the upper jaw and, if significant tissue grinding is necessary, move on to the lower teeth of the same name. After grinding the upper teeth, wax is applied to them and the dentition is achieved in distal occlusion. If there are areas of depressed (perforated) wax, the previously noted premature contacts on the distal slopes of the buccal cusps of the lower molars and premolars are ground off.
Elimination of premature contacts during anterior occlusion. Anterior occlusion occurs during the process of biting food. To identify supracontacts during the marginal closure of the anterior teeth and the movement of the lower jaw from the central occlusion to the anterior one, double-sided copy paper is used. The patient is asked to slowly move the lower jaw forward without opening the dentition. Anterior occlusion and forward excursion of the mandible are controlled visually and using carbon paper. The cutting edges of the lower incisors slide along the palatal surface of the antagonists. Having achieved marginal closure, the patient should open and close his mouth several times, holding a strip of double-sided copy paper between the front teeth. In areas of premature contact, carbon paper will leave a mark (imprint).
Selective grinding begins with the upper teeth. The cutting edge of the incisors and canines is ground (static phase of anterior occlusion), as well as the palatal surface of the upper incisors along the incisal path (dynamic phase of forward excursion of the lower jaw). The protruding teeth are pre-shortened. If pain appears in the area of the upper front teeth, due to the proximity of the pulp, or for aesthetic reasons, you can proceed to grinding off the corresponding antagonistic areas. Shortening the cutting edge of only the lower anterior teeth is unacceptable, as it leads to their separation from the upper incisors in central occlusion. After some time, the shortened teeth move out of the alveoli, which, in turn, aggravates the functional overload of the periodontium and the course of the pathological process.
During selective grinding of anterior occlusion, wide, flat incisal contacts should not be created. The cutting edges should be sharpened to natural sizes.
Elimination of premature contacts in lateral occlusion. To identify supracontacts, it is best to use double-sided copy paper. Analysis and selective grinding of supracontacts should be carried out on each side separately. It is recommended to start on the right side. To do this, copy paper is placed on the right side. The patient is asked to close the teeth and, without opening them, move the jaw to the left. When the dentition of the lower jaw slides to the left, supracontacts in the form of carbon paper imprints are revealed on the right side. The latter are usually localized on the vestibular slopes of the upper palatal cusps and the oral (lingual) slopes of the buccal cusps of the lower lateral teeth. Once the premature contacts on the right (balance) side have been eliminated, selective grinding can begin on the left side.
In the process of selective grinding on the balancing side, sections of the slopes of the cusps of the teeth that prevent the movement of the lower jaw from central to lateral occlusion and back are eliminated. At the same time, the zones that maintain the height of the bite, i.e., the tops of the tubercles, are preserved. If it is necessary to remove a significant layer of hard tissues of the teeth of the upper jaw, you can partially grind off the corresponding areas (oral slopes of the buccal cusps) of the lower lateral teeth. After eliminating the supracontacts on the balancing side, selective grinding on the working side begins.
Based on clinical observations and experiments, many experts recommend grinding the buccal cusps of the upper lateral teeth and the lingual cusps of their antagonists. In the specialized literature, this rule is usually denoted by the Latin letters BOLU (Buccal, Ober, Lingual, Unter), which means upper buccal and lower lingual. Grinding begins with the buccal cusps of the upper molars and premolars, which serve as guiding inclined planes (tangent) for the lateral movements of the lower jaw. The optimal type of grinding is considered to be one in which the lateral (transversal) movements of the lower jaw are carried out smoothly and unhindered. In this case, on the working side the bumps of the same name are in contact, and on the balancing side they are of opposite names or there is no contact.
When selective grinding in lateral occlusion, in addition to eliminating premature contacts on molars and premolars, it is necessary to pay special attention to the occlusion of the canines of the upper and lower jaws on both sides. If, when the lower jaw is shifted to the right or left side, only the fangs are in contact, and the remaining teeth are separated, then it is necessary to take into account the magnitude of such separation. In the initial stages of the disease, slight separation of the dentition (within 1-1.5 mm) is acceptable. In case of large separation, the canines should be shortened and smoothed so that with right and left lateral occlusions, multiple contacts of molars and premolars occur on the working side. If it is necessary to significantly shorten the canines, they are first depulped.
Selective grinding of teeth is carried out using a water-cooled turbine drill and a conventional drill. A special set of tools and materials for this procedure includes diamond and carborundum heads of various sizes and shapes (spherical, flame-shaped, umbrella-shaped, torpedo-shaped, cone-shaped, etc.).
Once sanding is complete, the surfaces are carefully smoothed and polished using fine-grain carborundum sockets, waterproof abrasive paper pads, and hard and soft rubber polishing tools. Selective grinding is carried out over several visits (3-5) with an interval of 5-7 days. Each of them should not exceed 30 minutes. At each return visit, a thorough follow-up examination of previously ground teeth is necessary to identify and eliminate residual premature contacts.
After selective grinding is completed, the surfaces are coated with fluoride varnish (preferably 2-3 times at intervals of several days).
Possible complications
If the rules for the procedure are not followed, the following complications are possible:
- decrease in interalveolar height;
- tooth displacement;
- hyperesthesia of hard tissues;
- excessive load on the periodontium after flattening the cusps of the teeth;
- removal of some teeth from occlusal contact and overload of the periodontium of others.
Therefore, the procedure can only be trusted to a dentist who has undergone special training and has the appropriate qualifications.
Methods for diagnosing supracontacts
The need for grinding is determined, usually during normal inspection.
If necessary, the following techniques are used:
- An occludogram is a technique in prosthetic dentistry that is used to identify and mark premature contacts on a wax plate. Used to monitor changes in treatment over the entire period. As a rule, the results of the first and last methods are saved.
- Diagnostics of jaw models - special impressions of the lower and upper jaws that reproduce its movement. Thanks to this, the doctor receives information about the shape/deformation of the arches, the nature of the deformation, occlusal contacts of the cusps, and sizes. It is carried out before and after sanding to determine the correct result.
- Marking with carbon paper is considered one of the most accurate and at the same time the simplest method for diagnosing supracontacts. A small piece of copy paper is used (approximately 3*4 cm), which is folded into 4 layers. The most suitable method for identifying contacts during mandibular dynamics.
- As an addition, you can use auscultation - a technique for examining the oral cavity, with the help of which certain sound vibrations are determined. In such cases, a bifurcated, dull sound or click is detected.