Timely treatment of caries in baby teeth is even more important than treatment of permanent teeth. And that's why:
- Normal eruption of permanent teeth and bite formation largely depend on the health and timely replacement of baby teeth. A complete set of primary teeth forms the correct jaw dimensions. If they are destroyed by caries and fall out or are removed ahead of time, then the jaw may not form as desired. This is highly likely to lead to malocclusion in the future or crooked teeth and unsightly alignment. As a result, a child, having matured, will pay for untreated caries in a baby tooth, at best, with braces, at worst, with teeth in a checkerboard pattern and psychological complexes. Losing (or removing) baby teeth too quickly can easily lead to malocclusion in the future.
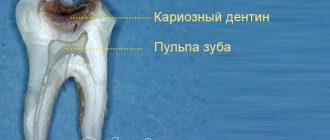
- Caries on baby teeth can be complicated by pulpitis and periodontitis, which can cause cysts to appear in the root zone, as well as damage to the permanent tooth germ.
- Advanced caries is often a reason for ridicule in children's groups.
- Also, do not forget that the appearance of caries is a sign of poor oral hygiene, an incorrect diet or a lack of minerals in the diet, and sometimes a symptom of problems with the immune system. If you ignore these problems at the beginning of life, then by the middle of his life the child may arrive without healthy teeth at all and with a set of concomitant diseases.
- If chewing baby teeth are removed early, the child will not be able to chew food normally. As a result, an insufficiently processed food bolus will enter the gastrointestinal tract, which can lead to digestive disorders
Often parents do not treat even serious forms of caries complications, and periodontitis in a child can turn into periostitis, osteomyelitis, abscess or phlegmon. Moreover, the level of deaths among children from complications of caries is higher than in adults, since with certain factors that weaken the immune system, the process from pulpitis to abscess and phlegmon in a child can take a matter of days and even occur within 24 hours.
Do baby teeth all change?
The child has 20 baby teeth. In an adult, the number of teeth can range from 28 to 32. Which baby teeth fall out? Everything! Normally, by the age of 14 they should change to permanent ones. Some teeth initially emerge as permanent teeth.
The order of loss corresponds to the order of appearance of baby teeth - the incisors change first, then the first and second premolars, and the canines change last.
The first molars grow permanently before the teeth change. Second molars appear in empty spaces created by jaw growth. Third molars (wisdom teeth) have lost their functionality and in many people do not grow back at all.
Children's teeth. Silver plated, filled or what to do?
Authors : Solovyov D.V.
Quite often you hear the phrase from parents: “The child has a hole in his tooth, they silvered it for us and sent us to wait.” In general, among parents (unfortunately, often under the influence of pediatric dentists) there is a widespread opinion that all treatment of baby teeth usually comes down to “silvering” and waiting. On the one hand, this dulls vigilance: they say, if something happens, we can easily do this very quick procedure and we won’t know grief; on the other hand, it discourages unnecessary visits to the doctor: not everyone likes the result of this action in the form of black teeth (especially on a girl ). So what is this notorious silvering?
Silvering is the lubrication of a tooth with a special composition, resulting in a layer of restored silver remaining on the surface. The point is that this layer should, in theory, exhibit disinfecting properties and prevent further spread of the process.
Silvering seems to be a rather convenient way of prevention - it is done quickly, the child does not have time to get tired, the dentist is able to serve quite a lot of patients. However, our mass passion for silvering is not at all healthy. The most important thing to understand is that silvering is only an attempt to preserve the process, and not a treatment at all. That is, this attempt may or may not be successful; in fact, we rely on luck. In addition, under the layer of black silver it is not visible how far the process is spreading. As a result, too often the tooth happily rots further, while the parents think that everything is fine.
Why do doctors very often say that nothing can be done and we have to wait? Yes, because in our country treating children is a completely unprofitable business. In the public service, a strictly defined time is allocated for treatment, while the personal characteristics of the child are not taken into account at all (i.e., is it necessary to persuade him), the nurse, as a rule, does not work in tandem with a specific doctor, there is simply not enough modern materials and conditions for quality work. Commercial children's services are literally at odds for another reason - treatment of children is much more expensive than an adult, and in our conditions there are not many people willing to pay such an increased price. That is why it is much easier to “anoint and send away” in half a minute.
It must be said that abroad, even prosthetics for children is a completely common, routine matter. For us, it seems like some kind of almost space technology.
What's the best thing to do?
— Silvering is permissible only at the initial stage of the process . If after a month or two it is clear that the process does not stop, see the next point.
— If there is already a cavity (and not just a stain), then it is necessary to fill it. No better drills have yet been invented, especially in comparison with various “laser treatments” or “treatment without drilling.” The laser has quite a few limitations, and no chemical can clean out rotten cavity as well as a drill, although the choice is certainly yours.
— A rotten tooth is a source of infection. Removing baby teeth too early is certainly not a good option. But if a baby tooth has already disappeared “to the ground,” then we need to evaluate which evil is less – a chronic source of infection (which can also affect permanent teeth) or a hypothetical (i.e., which may not exist) uneven teeth in the future. In order to save space for the future permanent tooth, there are so-called “space keepers”.
— Statements that “baby teeth cannot be treated” are a blatant lie ! They not only put fillings (and normal ones at that), but also remove nerves and fill canals (although not quite the same as for adults).
— If it is not possible to establish contact with the child (it is not possible), and more than one tooth needs to be treated, then the best option is anesthesia. Don't be afraid of anesthesia, it is completely different now than it was 20 years ago. In addition, the harm from the psychological trauma of a screaming and struggling child will be much greater. Not to mention the pain and risk of serious injury if the child twitches. Just in case, the turbine installation produces a minimum of 300 thousand boron revolutions per minute.
— A really effective prevention is the so-called fissure sealing. This is a coating of teeth (we are talking about still healthy teeth, not already missing ones) with a special composition (like white varnish), which hardens under the influence of a special lamp, “smoothes out” tooth irregularities and releases fluoride (which increases the tooth’s resistance to caries). Lasts for at least six months (usually more). I would like to draw special attention to the fact that using a drug called “fluoride varnish” is far from the best option. This is a very cheap domestic varnish that hardly hardens on the tooth, is almost completely washed off the tooth within a few hours, but it holds up remarkably well if it gets on clothes.
— The teething dates are written here.
Please note once again that deviations from these deadlines by 6 months in one direction or another are the norm! The order of cutting is arbitrary and most often does not play a special role!
The choice, as always, is yours.
Consultations by Dmitry Solovyov at ClubCom
published 03/09/2013 11:36 updated 27/09/2016 — Diseases of the teeth and oral cavity, Dentistry
"Shark Teeth"
During the process of root resorption, baby teeth become loose and, pushed out by growing permanent teeth, fall out. But sometimes the mechanism of this process fails. The permanent tooth has time to grow before the milk tooth that precedes it falls out.
Sometimes a whole row of such permanent teeth grows parallel to a row of milk teeth, which, for some unknown reason, do not fall out. Such teeth are usually called “shark” teeth, by analogy with the dentition of sharks, in which the teeth grow in three rows.
Studies have confirmed that “shark teeth” do not cause problems in the long term. When a baby tooth falls out, the “shark tooth” begins to shift and takes its normal place.
Dental treatment for children: yesterday and today
Just 15-20 years ago, finding a specialized clinic or specialized specialist for a child was quite a difficult task, especially in small provincial towns. Children often had to be treated in places where sometimes even minimal comfort was not provided, which is why many children subsequently suffered from dental phobia. Today the situation has changed dramatically: many private high-class pediatric or family dentistry clinics have appeared, which provide a decent level of treatment and service. The main problem today remains the rather low information awareness of patients, which is why many children do not receive timely treatment and have all sorts of complications.
For example, many parents seriously believe that it is not necessary to treat baby teeth, because they will fall out in any case, so often the child ends up in the dental chair when it is not possible to save the tooth. Of course, this approach is fundamentally wrong. Under the milk teeth are the rudiments of molar teeth, so early loss of temporary teeth or extensive infections threatens a number of complications: from impaired development of permanent teeth to serious dental anomalies. The summary here is obvious: you need to monitor your dental health and eliminate problems in a timely manner from a very early age. Of course, dental treatment for children of different age groups has its own characteristics, so let’s take a closer look at the specific nuances.
Make an appointment
right now!
Bandina Ekaterina Dmitrievna
Pediatric dentist
Anesthesia for dental treatment in children
Anesthesia for children during dental treatment is carried out using the same technologies as for adults, but only in smaller dosages of drugs.
| Pain relief techniques | Description |
| Local anesthesia | Local anesthesia is divided into two subtypes: with the administration of drugs by injection (infiltration anesthesia) and without the use of a needle and syringe (application anesthesia). Painkillers for dental treatment are administered to children using both methods. Application anesthesia is gels with different tastes and odors, which are used to treat the oral mucosa in the area of intervention. |
| Sedation | Sedation is the safest and most comfortable technology, one of the most common and popular pain management techniques in pediatric dentistry. Using a mask, a mixture of nitrous oxide and oxygen is supplied, which relieves anxiety and relaxes the child. Sedation using propofol is a drug-induced sleep where the drug is administered intravenously and is used for patients over 15 years of age. |
| General anesthesia | Anesthesia in dental treatment in children is used less often than other methods. Complex clinical cases are treated under general anesthesia when large-scale and long-term treatment is required in one session. In addition, general anesthesia is performed for children with mental and neurological problems. Inhalation anesthesia is carried out using a mixture of sevoran and oxygen, also with the use of a mask, which can also be classified as medicinal sleep. For all types of general anesthesia, a numbing injection is used before treatment. |
Dangerous symptoms!
After dental treatment, the temperature in children may increase by 1-1.5 degrees. If it does not return to normal within a few days, you should consult a doctor who can prescribe appropriate medications. Never give your child antibiotics or strong antipyretics without the approval of a specialist.
Features of treatment of baby teeth
Carious lesions of primary (temporary) teeth are widespread. The progression of dental damage in childhood and preschool age is observed in all countries of the world. The difficulty in treating caries in primary teeth lies not only in the anatomical and physiological characteristics of the child’s primary teeth and oral cavity, but also in the difficulty in adopting the right strategies when working with a child patient. This often leads to the development of complications of caries and premature removal of baby teeth, which in turn negatively affects the rudiments of permanent teeth, general health and can lead to the development of odontogenic inflammatory processes in the maxillofacial area and anomalies. That is why the problem of treating caries in childhood is especially acute.
Getting children and parents overcoming their fear of dentists is also an important aspect. Since the sound of a working dental unit is a powerful factor in the development of dental phobia, special attention is paid to creating a noise-free, “friendly” way to treat caries, especially in childhood. However, many modern treatment techniques (ozone therapy, laser or ultrasound preparation) have proven to be of little effectiveness in young children. Some other methods also have their drawbacks and do not always lead to good results. And the silvering procedure, for example, stains the teeth black, so many parents refuse it. In addition, silvering also causes many complications in the future.
Atraumatic restorative treatment of childhood caries and chemical-mechanical preparation of carious cavities have become the most promising techniques in pediatric dentistry. There is insufficient information in the literature regarding the use of these techniques in pediatric practice, the types of preparation and their impact on the behavior of children, and the indications and contraindications of these techniques are not clearly clarified.
In cases of deep caries, it is recommended to use a protective calcium-containing lining or perform a thorough fluoride treatment of the roof of the pulp chamber. This technique is rarely used in primary dentition, as it is believed that primary teeth are not often affected by deep caries. But on the other hand, the hard tissues of primary teeth have specific anatomical and physiological characteristics that contribute to the rapid spread of infection and the development of complications from small carious cavities. Treatment of intermediate caries protects the pulp and accelerates the mineralization of damaged dentin. In such cases, the use of fluoride compounds is recommended, although their reliable effectiveness remains unknown. Glass ionomer cements are used to restore primary teeth. In recent years, the treatment of caries with light-curing materials in primary teeth has been carefully studied by researchers. Although the justification of aesthetic restorations in primary dentition remains unproven, some other techniques for treating secondary caries in childhood are also poorly understood.
Object of study
Rationale for exhaustive therapy in the course of treatment of secondary caries of primary teeth in children aged 1-5 years.
The following tasks were identified:
1. Assess the behavior of children aged 1-5 years during various cavity preparation techniques
2. Compare the quality of various preparation techniques in children aged 1-5 years.
3. To identify the positive effect of using fluoride to treat the roof of the pulp chamber in children
4. Assess the justification of aesthetic restoration in children aged 1-5 years and establish the effectiveness of the light-curing materials used.
5. Develop the most effective and comprehensive method of treating primary teeth and find out its effectiveness in the age group of 1-5 years.
Scientific novelty of the research
The behavior of children in terms of the technique chosen for tooth preparation is examined for the first time. It has been proven that the use of atraumatic methods and chemical-mechanical preparation of carious cavities has a beneficial effect on the behavior of children, while the use of a dental unit affects the development of a deliberately negative attitude of children towards dental procedures. A comparative study of various preparation techniques (standard, atraumatic, chemical-mechanical) using a caries detector in children aged 1-5 years has not been conducted before. The use of a caries detector is necessary to assess the complete removal of carious dentin when using any of the preparation techniques. The use of fluoride to treat the roof of the pulp chamber of temporary teeth has shown its high efficiency. The need for aesthetic restoration of primary teeth in childhood has been established. The clinical effectiveness of treating moderate caries using light-curing glass ionomer cements has been revealed. A comprehensive technique for the treatment of caries in primary teeth has been developed, tested and then evaluated. The effectiveness of this method was 94.8% compared to the conventional method, which showed 83.5%. The study was conducted with the participation of children aged 1-5 years.
Scientific and theoretical significance of the study
The theoretical significance of the study was to obtain new information on a comparative analysis of various methods of preparing primary teeth in children, the effect of preparation on the behavior of children during this procedure, the need for aesthetic restoration of these teeth, the importance of using fluoride to increase the effectiveness of therapy.
The practical significance of the study lies in the development of a comprehensive and effective method for the treatment of caries in childhood. The need to use a caries detector is determined by the assessment of adequate preparation.
Research abstract
1. The behavior of children during oral sanitation measures significantly improves when using atraumatic and chemical-mechanical preparation techniques. While the use of conventional dental units causes negative emotions in children.
2. The use of a caries detector was carried out to assess the completeness of removal of infected tissue and the quality of preparation in all applied methods
3. The use of fluoride to coat the roof of the pulp chamber increased the effectiveness of therapy for primary teeth in children.
4. The exhaustive technique increased the effectiveness of treatment of moderate caries in primary teeth of children aged 1-5 years compared to the traditional technique.
Approbation of research results. Implementation of discoveries. Publication of abstracts.
The research materials were presented and discussed at the conference of young scientists of Volgograd State Medical University (2004-2006), the XI regional conference of young scientists in the Volgograd region (Volgograd 2005), the VI international scientific conference “Health and education in the third millennium” (Volgograd 2005).
The study was also announced at a meeting of pediatric, therapeutic, surgical, and orthopedic dentists in Volgograd State Medical Academy (September, 2006).
According to the established goals and objectives, a multi-stage study was launched. 448 children aged 1-5 years took part in it. The children were formed into groups according to gender and age.
Research base
Municipal children's clinic No. 2 in Volgograd. Participation in the study was voluntary. Informed consent for children's participation was obtained from their parents. The study protocols were approved by the regional ethical community. At the first stage, the attitude of parents (192 families) to various methods of preparation of baby teeth, as well as the behavior of children in the process of sanitation, was determined. 47 children underwent standard preparation techniques for primary teeth, 48 underwent atraumatic preparation, and 97 underwent chemical-mechanical preparation. Standard technique was performed using a dental unit, high and low speed handpieces, diamond, carbide and steel burs. The atraumatic method of preparation was carried out using the ART technique (Pakhomov, Leontyev 2004). The chemical-mechanical method for preparing the carious cavity of temporary teeth was carried out using the preparations “Carisolv”, “Medteam”, Switzerland. Glass ionomer cement was used for filling. Children's behavior during sanitation was recorded during the first four visits.
Criteria for parental assessments regarding treatment of children
1. Satisfaction with the treatment experience, full agreement with the doctor on all issues.
2. Dissatisfaction with the treatment method chosen by the doctor for one reason or another. The need to change it.
Children's behavior was assessed according to the following criteria
1. Good: the child is sociable, trusts the doctor, sits well and opens his mouth calmly
2. Satisfactory: the child is difficult, restless and reluctant to open his mouth. For complete treatment, the help of parents and medical personnel is necessary.
The second stage consisted of a qualitative assessment of the process using a caries detector in 53 children. With the standard preparation technique, the detector was used in 30 cases, the atraumatic technique in 15, and the chemical-mechanical technique in 62. To determine necrotic dentin, the “Color-test” detector (VladMeVa) was used. Using this detector, adequate cavity preparation was assessed in different ways.
The third stage of the study consisted of fluoride treatment of the roof of the pulp chamber in 78 children, as part of the treatment of moderate caries in children (145 children). The standard technique was applied to 215 teeth. Deep fluoridation was carried out using a bonding agent (liquid sealant), “Humanchemie”, Germany. During the fourth stage, parents' opinions were obtained regarding the aesthetic component of treatment (according to a survey of 100 respondents), and the effectiveness of treatment of moderate caries of 56 temporary teeth in 23 children aged 3-5 years was assessed using various preparation methods and further restoration with light-curing materials Vitremer TM, 3M ESPE.
During the fifth stage, based on surveys, a comprehensive methodology was developed for the treatment of moderate caries in primary teeth of children aged 1-5 years. Treatment included: preparation of carious cavities (ART, CMP techniques), use of caries detectors to assess the quality of preparation, deep fluoridation of the pulp chamber after preparation, filling with glass ionomer cement. This algorithm was applied to 381 teeth in 142 children. The standard method of treating moderate caries (preparation using a dental unit, filling with GIC) was used in the same group of children on 315 teeth. The localization of carious lesions in different techniques was approximately the same. After 18 months, the effectiveness of the exhaustive technique compared with the standard technique was established. To evaluate the results of treatment of average caries of temporary teeth, the following parameters were taken into account: the presence or absence of complications after treatment (pulpitis or periodontitis), secondary lesions, quality of filling according to the anatomical shape, preservation of the tooth surface and gingival attachment.
After the examination, the quality of treatment was assessed:
1) positive result: the filling restores the anatomical shape of the tooth, preserving the gingival attachment or the presence of a small defect without involving dentin, there are no signs of secondary damage or complications.
2) negative result: extensive damage to the filling, violation of the gingival attachment, uneven surface, loss of integrity, loss or abrasion of the filling, recurrent caries and complications.
All statistical calculations were carried out using an IBM Pentium 4 computer using software (Microsoft excel 2000). Marginal category (%), mean error (m), significance (t) and deviation (p) were reported. The deviation was considered statistically significant at t>2 and p
Research results
The interview results showed that the majority of parents had a positive attitude towards the need to treat their children and were satisfied with the doctor’s work. Only 4.2% of parents were dissatisfied with the experience. Regarding the behavior of children, the majority of patients from the standard treatment group (74.4%) showed a negative attitude towards therapy at the first visit, their behavior was unsatisfactory. Over the course of treatment, the percentage of children with a negative attitude towards treatment rose to 78.6%. By the second visit, the number of children with bad behavior increased by 12.7%, by the third - by 6.3%. By the fourth visit, no child was showing good behavior. Satisfactory behavior during standard preparation was observed in 21.4% of children. The majority (72.9%) of children showed good behavior with the ART method. Gradually, the number of children with good behavior increased to 93.8% by the fourth visit. The number of children with satisfactory behavior, which was 16.6% at the first visit, decreased to 2.1% at the fourth visit.
Bad behavior was observed in 10.5% at the first visit, the reduction in negative attitudes decreased and by the fourth visit it was already 4.1%. In the group of children in which chemical-mechanical preparation was used, good behavior was observed in 47.7%, its proportion increased to 52.5%, 74.2%, 97.9%, respectively, at the second, third and fourth visit. The number of children with satisfactory behavior was 27.8 and gradually decreasing, reaching 1% at the fourth visit. Also, the number of children with bad behavior decreased from 27.8% to 1% by the fourth visit. A comparative analysis of the results showed that children treated with ART and CMP techniques tolerated the procedure much easier than patients who underwent standard preparation. With the ART and CMP techniques, almost all children showed good behavior and attitude towards treatment, while with the standard technique, the opposite results were observed: the number of children with good behavior came to zero by the end of the procedures. Bad behavior and negative attitudes among children remained at a high level: 74.4% - 76.8%.
Qualitative assessment of the performed preparation of primary teeth.
The use of a caries detector revealed remaining infected dentin in all preparation techniques used. Although preparation defects were found more often (p
No statistically significant deviation was found during preparation using ART and CMP methods (13.3%+-8.8% and 24.2+-5.4%, p
Pros and cons of various techniques.
The rapid removal of infected tissue may be considered an advantage of the standard dissection technique. At the same time, the use of a drill leads to the development of a negative attitude and increases the level of dental phobia among the population. The ART method has significant advantages due to quiet, gentle cleansing of the cavity, minimal risk of opening the pulp chamber and damage to surrounding tissues, reducing fear and anxiety in children and their parents. However, this technique is applicable only to “open” cavities; it cannot remove all altered dentin. In addition, careful excavation can lead to infection of the dentin near the pulp horn and the enamel-dentin junction. Also, this technique takes quite a long time.
Advantages of CMP: painless and quiet procedure, comfortable implementation for children and parents, safe for the oral mucosa, maximum preservation of healthy tooth tissue, easy removal of affected tissues after softening with gel, the ability to manually expand the enamel boundaries, allowing you to create a sufficient cavity. Disadvantages of the technique: it is not always possible to open the cavity with a hand instrument, the gel may not always be effective in softening dentin, manual removal of carious dentin from the medial wall of the cavity of primary molars is ineffective, some children note an unpleasant odor of the drug, the time of extraction of carious tissue increases. The use of fluoridation of the roof of the pulp chamber before filling showed good results (Figure 3). A positive result after the procedure was observed more often than in the conventional technique 94.5%+-1.9% and 82.8+-2.6%, respectively, p
The problem of aesthetic filling of temporary teeth.
According to the results of a survey of parents, the majority of respondents (about 73%) consider it necessary to carry out aesthetic treatment for their children. 17% reported that they considered aesthetic treatment an advantage and 10% were undecided. At the same time, 33% are ready to choose a treatment method on their own, 60% completely rely on the doctor, and 7% find it difficult to answer. A small number of families (21%) can also choose their own filling material. On the other hand, the choice of therapy technique is also limited by the family budget. Despite this, 80% are considered to be families with a good income, most of them prefer free medicine (17%) or cheap treatment for caries of primary teeth (49%). Only 34% of respondents decide on aesthetic treatment for their children.
The use of light-curing materials in pediatric practice is limited by certain difficulties: the need to work with 4 hands, more time is required for treatment, the child must be calm and follow the doctor’s instructions, good isolation of the area from oral fluid. According to this, filling is very difficult in children under 3 years of age, in children who are not sociable, in active and inquisitive children who cannot sit quietly with their mouths open for a long period of time. Repeated examination of children after 12 months revealed that satisfactory results of using Vitrmer after the CMP technique were observed in 87.8%, after ART - 84.6%, after CP - 80%, the number of negative results -12.2%, 15.3% , 20.0% respectively. However, the deviations were found to be statically unstable (p0.05). The limitation on the use of light-curing materials is, on the one hand, due to the low aesthetic requirements of parents and their economic resources, and on the other hand, the complexity of the work associated with the behavior of children.
Comprehensive treatment of moderate caries of primary teeth in children.
Exhaustive therapy according to the study results includes preparation with CMP and ART techniques, use of a caries detector to assess caries excision, application of sealants to the pulp roof, and GIC filling. After the described treatment, positive results were found 18 months later in 94.8% of cases, after the standard method - 83.5% (p0.05), class III - 1.9 times less (17.9+-6.1% and 34.0+-6.7%, p>0.05), class IV – 6.2 times less *2.6+-1.5% and 16.1+-4.7%, p
Thus, the method of exhaustive treatment is recognized as the most effective and desirable for implementation in clinical practice.
conclusions
1. The behavior of children during oral sanitation depends on the chosen preparation technique: the use of new techniques (ART and CMP) leads to the formation of a positive attitude towards the treatment process in 93.8% -97.9% of cases. When using standard dissection techniques, a negative attitude is observed in 78.6% of children.
2. It is recommended to determine the quality of preparation of the carious cavity of primary teeth using a caries detector: this is especially effective when using the ART and CMP techniques. Preparation defects using the standard method are determined 2.8 times less than with chemical-mechanical preparation and 5 times less with atraumatic preparation.
3. Deep fluoridation of the roof of the pulp chamber significantly increases the effectiveness of treatment of moderate caries of primary teeth. The number of unsatisfactory results during fluoridation is reduced by 4.2 times compared to the standard method: 5.5+-1.9% and 17.2+-2.6%, respectively, p
4. The need for aesthetic treatment of children aged 1-5 years is 34%. The effectiveness of Vitremer is 85.5%, negative experience is 14.3%, which approximately corresponds to the data on GIC fillings.
5. Exhaustive treatment of caries, including preparation using ART, CMP techniques, the use of a caries detector, deep fluoridation of the roof of the pulp chamber and GIC filling is recognized as preferable. The use of this technique in children 1-5 years old increases the effectiveness of treatment by 11.3% compared to standard treatment: 94.8% and 83.5%, respectively, p
Practical recommendations
1. In the process of rehabilitation of children aged 1-5 years, it is recommended to adhere to the following recommendations:
— ART technique is recommended for active and restless children under 3 years of age, preschool age, experiencing severe anxiety and fear, and also having good access to the carious cavity
-CMP technique is recommended for children under 3 years of age, children of any age to establish a trusting relationship with the doctor, patients with a fear of the sound of dental equipment and injections, with a burdened allergic history, emotional instability and mental disorders.
- standard preparation techniques can be used for emotionally stable children, school-age children who are calm about the dentist’s manipulations, including anesthesia. If there is no good access to the carious cavity, the described techniques should be combined.
2. At the final stage of preparation, regardless of the chosen technique, you should use a caries detector to determine the quality of excision of affected tissue. It is necessary to ensure the absence of intense staining.
3. Treatment of moderate caries of primary teeth in children aged 1-5 years is recommended to be carried out using fluoridation of the roof of the pulp chamber, this significantly increases the effectiveness of therapy.
4. For the greatest treatment effect in children 1-5 years old, it is necessary to resort to an exhaustive treatment method, including all the stages described above, including GIC filling.
Author:
Dr. Dina Jafar Mohammad