Composite dental restoration is the restoration of anatomical shape using light-curing filling materials. The technique has its advantages and disadvantages. Light-curing composite is one of the most popular and widespread materials for therapeutic treatment and microprosthetics. The most modern option is hybrid composites, which have excellent strength, adhesion to the surface of the teeth and give minimal shrinkage during polymerization.
How restoration is carried out using the direct method - a step-by-step description of the process
To better imagine how the restoration procedure occurs, you need to understand how it is done using the direct method. If the indirect method involves the separate production of dentures using impressions and their subsequent fixation with adhesive or implant, then direct restoration is carried out directly in the patient’s mouth. The process includes the following steps:
- preparation of the oral cavity: removal of deposits, elimination of foci of inflammation and tissues destroyed by carious processes,
- selection of material by color and degree of transparency,
- administration of an anesthetic: anesthesia is used when large-scale work is to be done, including the installation of a pin or stump inlay - before this, the nerve is usually removed and the canals are filled,
- preparation: grinding the defect area, removing affected tissue, making a small indentation for better fixation of the composite material,
- isolation from saliva using a rubber dam: a small latex pad with a hole for the tooth is fixed in the working area,
- fixation of a pin or stump inlay in the canal: carried out when more than half is destroyed, after removal of the nerve, treatment and filling of the canals,
- treatment of the surface of the support for better adhesion: with the help of special compounds it is dried and made slightly rough for reliable adhesion to the photopolymer,
- Layer-by-layer application of light-curing material: each subsequent layer is illuminated with a special UV lamp, under the influence of which it hardens. This technology makes it possible to achieve maximum strength of the composite fastening and accuracy in reproducing the anatomical shape.
In some cases, taking impressions is required to correct the problem.
Upon completion of all manipulations, the restored area is ground and polished. As for how long the entire procedure takes, everything is purely individual: from half an hour to hide a small chip to several hours to build up most of the damaged crown.
Types of artistic dental restoration
Direct method
If the damage is minimal, then doctors decide to use a direct restoration method. This method allows you to solve the problem in one procedure. So it is in high demand.
For the direct method, photocomposites are used. The material is easy to use and very durable. To proceed to direct restoration, it is necessary to first carry out diagnostics, then cleaning, and anesthesia. Although dental restoration using the direct method is carried out in one session, there are still several stages of work.
The dentist will not be able to proceed to direct restoration until he determines the scope of work and chooses the necessary method to solve the problem. It is impossible to do without professional cleaning. For filling, photopolymers are used, the color of which is selected after cleaning.
Indirect method
This method is also called external. The indirect method is characterized by the use of orthopedic structures. Most often, a veneer is used for this - this is a thin plate for the manufacture of which ceramics is used. The material is excellent for cosmetic tooth restoration. Indirect dental restoration allows you to eliminate the most complex defects: large gaps, carious deposits.
Composite dental restoration
Filling is carried out using photopolymers in several layers. No grinding is required to perform a composite restoration. If the tooth was not treated before restoration, the old filling may need to be removed.
Composite restoration can be compared to veneers; the enamel surface remains intact. 2 grooves are drilled on the surface. Polymers are installed in them. Then a special composition is applied. It will degrease the enamel and eliminate pathogenic microbes. Only then does the doctor apply photopolymer. An even thin layer is dried using a special lamp. Then you can apply the next layer. The number of layers will be determined by the doctor.
Composite restoration is used to eliminate minor defects: chips, cracks, wide gaps. It is not possible to restore chewing function with polymers. The composite procedure is also called artistic restoration of teeth.
Pin installation
To improve the connection between the filling and the tooth, medical pins are used. They are made of titanium, gold, metal. The cost of the restoration procedure will depend on what material was used for the pins. The pin is installed quickly, without pain. The pin can be placed in the front teeth and canines.
The tooth is cleaned, then the root canals are drilled, and then a solution is poured into them for the filling. At the end a metal pin is installed. When the fixing solution has hardened, you can build up the missing part. Taking into account how badly the original crown is damaged, an inlay can be installed. At the end of all work, grinding and polishing must be carried out.
Prosthetics with crowns
When installing a crown, it is not necessary to remove the affected tooth. But you will still have to clean the root canals and remove the nerve. Thus, it is possible to reduce the risk of inflammation. Bacteria can leak onto the surface that is ground down for the crown. If there is caries, then it should be cured, just like gum disease. If this is not done, it is simply impossible to carry out reconstruction.
After the nerve is removed, an impression is made. Various materials are used to make crowns. If aesthetic restoration of teeth is necessary, then metal-ceramics or ceramics are used. Thanks to these materials, it is possible to give the prosthesis a shade that perfectly imitates the color of the natural one.
The installation of a crown can be completed after 3 visits to the doctor. After the impression has been made and the crown has been made, the tooth will have to be ground down. It must be reduced on all sides. As a result, it should look like a thin, low stump.
Veneers and Lumineers
Veneers and lumineers are practically the same thing. You do not need to remove the nerve to use this method. When installing such structures, minor grinding of the teeth is performed. The surface is ground down to the thickness of the veneer. Then the denture will not stand out in the dentition. With the help of veneers, it is possible to visually make teeth larger, so they are used mainly on the front ones to remove gaps or correct their shape.
Thanks to veneers, it is possible to lighten the enamel by a couple of tones when conventional whitening methods do not help. Lumineers are thin and light. So there is no need to grind the enamel. If desired, the lumineers can be removed in the clinic after some time. Lumineers are attached using a fixing gel. It contains strengthening fluoride.
Care after composite restoration
To maintain aesthetics as long as possible, teeth require especially careful care. It is better to quit smoking and minimize the consumption of foods that are potentially harmful to the color of teeth, such as tea, wine, and food with dyes. It is important to have it professionally cleaned regularly. Thorough brushing of your teeth with a toothbrush should be done at least twice a day. It is also advisable to use dental floss and special rinses.
Author:
Mayorov Andrey Mikhailovich
Specialization:
orthopedic dentistry, dental prosthetics, implant installation
What is direct and indirect restoration?
It's actually simple. Direct restoration is performed in one day and directly in the patient’s mouth. Indirect, on the contrary, requires more time and is carried out using a laboratory.
Direct restoration is perfect for those who urgently need to restore the appearance of their smile. Chips of hard tissue, as a rule, occur unexpectedly, and there is not always time to wait until crowns and veneers are made for you. Of course, such a restoration has its drawbacks. First of all, this is a low service life. After such a recovery, many resort to a more long-term recovery. Indirect dental restoration lasts at least 2-3 visits to the dentist. Each product is made according to individual parameters in a special laboratory. Sometimes such restoration is used in cases where the appearance of the smile has only minor defects.
General overview
The material, which is based on a nanocomposite mixture, combines a whole list of heterogeneous microelements, while the percentage of filler content in them is at least a third of the declared volume. The basic components used for the manufacture of the compositions under consideration include quartz, heavy salts, titanium and zirconium silicate, metal oxides, and crystalline polymers.
The universal specificity of materials determines the range of options for their practical application. Within the dental field, nanocomposites are used as:
- Basics for the manufacture of filling inlays that restore the structure of crowns;
- Material that masks areas of enamel that have undergone erosive changes;
- Corrector of anomalies that arise during the development of elements of the dentition;
- A composition that temporarily replaces the prosthesis when restoring chipped areas;
- An insulator or sealant that prevents tissue infection.
The production of compositions containing microelements requires the organization of complex production, which provides for the option of point optimization, modification and production of true nanocomposites based on their own structural carriers.
Strength of dental restorations and care recommendations
After the procedure, the patient is advised not to eat for two hours and, in general, to abstain from solid foods that require intense chewing for 24 hours. The color fastness of restorations in the first 24 hours leaves much to be desired, so you should not drink strong tea, coffee, colored drinks and berries, and women should not wear bright lipstick. Restored teeth require strict adherence to the rules of oral hygiene. With insufficient care, marginal pigmentation quickly appears (also appears when smoking), shine is lost, and the risk of caries increases.
The quality of direct artistic or composite dental restoration can be assessed according to the following criteria:
- Correspondence to the anatomical shape of the tooth being restored
- Absence of a tactilely defined boundary between artificial and natural tooth tissues
- Healthy gum condition in the area of the restoration performed
- Absence of a white or gray line along the edge of the restorative material
- Lack of postoperative sensitivity
- Matching the color of the restored surface to the natural shade of the tooth
- Presence of surface gloss
- Absence of pores and white lines in the thickness of the restoration
How long will composite fillings last?
All composite restorations tend to darken over time. For bulk fillings, the problem of wear and chipping also arises. Research in recent years shows that within five years, about 15% of composite fillings required some degree of restoration. However, none of them were completely lost; only minor cosmetic “repairs” or polishing were required.
Clinical actions when identifying the lack of adhesion of a portion of the composite
Direct dental restoration
Direct restoration of chewing teeth and the frontal group is carried out in the patient’s oral cavity. This became possible thanks to the invention of photopolymer composites. Modern light-curing materials have a rich palette of shades and a natural level of transparency, thanks to which the restored tooth does not differ in appearance from others in the dentition.
The main advantage of the direct restoration method is that all manipulations can be done in one visit, while the production of veneers requires more time. An experienced restorer who has all the necessary skills for artistic restoration of anterior teeth can restore the entire frontal group of teeth in one day.
On average, filling or restoring one tooth takes from 20 minutes to 1 hour, depending on the complexity of the situation. Aesthetic restoration of frontal teeth always takes more time, since the material is applied in layers of different colors and densities, and the shape of the crown part is modeled. For naturalness, a translucent cutting edge of the tooth enamel is formed, and at the polishing stage, a surface microrelief is created with special tools.
A separate item is the restoration of crooked teeth with composite material. Many patients ask the question: is it possible to correct curvature without braces? In fact, this issue is always resolved individually and only together with an orthodontist.
With a slight curvature, it is possible to correct the defect with filling material if the contact with the antagonist tooth is acceptable. If the tooth protrudes strongly from the dentition, and its correction requires significant grinding of hard tissues, then the long-term results of such intervention may be unsatisfactory.
In recent years, composite materials have also become widespread in pediatric dentistry. Restoration of baby teeth in a child can be carried out after silvering, when the enamel of the teeth darkens and takes on an unattractive appearance.
Restoration of temporary teeth of the chewing group with cements did not show the desired results, while composite fillings are more durable and allow you to preserve the child’s damaged teeth until they are naturally replaced. Restoration of baby teeth in children is difficult to perform - for good fixation, complete isolation from saliva is required, which is quite difficult to achieve when treating children.
Modern methods of dental restoration using composite materials require certain skills from doctors and include several stages. After preliminary preparation and removal of carious tissue, an etching is applied to the treated surface - a gel based on orthophosphoric acid, and kept on the tooth for 25-30 seconds.
Then it is washed off, the tooth surface is dried and a special glue is applied - an adhesive that is responsible for adhesion of the material to hard tissues. The composite material is applied in small portions, each layer is illuminated with a special lamp.
For the restoration of one tooth, several shades can be used, in accordance with the color of dentin, enamel and transparent incisal edge. Dental restoration in children is usually carried out in one color.
Criteria for choosing a composite material for dental restoration
All modern composite materials are in demand by practicing doctors to one degree or another, but it is impossible to single out just one, the best. We choose a composite based on many criteria, but ultimately it all comes down to a “like it or don’t like it” decision. Any new material must be assessed according to at least two parameters, and then this choice will be objective.
First, you need to evaluate what aesthetic potential the restoration material you have chosen has. Doctors and patients always strive to ensure that treated teeth do not differ in appearance from healthy ones. To achieve this, the manufacturer completes sets of composites with materials of different colors and transparency. Having such materials, the dentist independently decides how to use them and what method to build the restoration. The quality of restoration depends on the clinical experience of the doctor and his manual skills. However, the aesthetic potential of different materials is not the same, and the doctor tries to choose what is right for him. Modern materials with wide aesthetic possibilities include the latest nano-composite from the SCHUTZ Dental Group – NanoPaq (Fig. 1). This material is a whole system, which includes flowable composites with different degrees of viscosity (NanoPaq Flow and NanoPaq FlowHard) (Fig. 2), a fifth generation adhesive (NanoPaq Bond), as well as specially developed diamond polishing pastes (NanoPaq Polish), but special Of interest is the simple and convenient system of color coding and transparency gradient of this material. NanoPaq – is divided into 4 groups with varying degrees of translucency (Fig. 3): 1. Opaque material (Opak-Universal - OU). This material is presented in a universal shade (A 3 - A 3.5), which is completely opaque (Fig. 4). When used, the opaque can cover any dark object, and the versatility of the color allows it to be combined with a composite of any color group. When applying layer-by-layer, it is advisable to place the material as deep as possible, since it can stand out as a light spot on the surface due to its high ability to reflect light. That is why for reliable polymerization with light it must be applied in thin layers. This is not difficult to do, since the material is fluid. Opak-Universal can be used to cover dark tooth tissues with a pronounced change in color (resorcinol-formalin and tetracycline teeth, amalgam staining, age spots, etc.). This material can be used to block the metal color of root posts or cast cores, as well as to disguise metal when repairing chipped porcelain.
2. Low-transparent materials (Opak-Dentins - OA, OV) Unlike the opaque Opak-Universal, Opak-Dentins slightly transmit light and are auxiliary materials. They help to reliably cover the gray background when restoring through holes in the anterior section. They work well in deep layers of restoration, reducing overall transparency and enhancing color intensity. In practice, two shades OA 2 and OA 3.5 (for light and dark teeth) are most often used (Fig. 5). Since these materials have a greater influence on the transparency and brightness of the restoration rather than on the color itself, they can be used for any color group according to the VITA scale. Available in three shades: OA 2, OA 3.5, OB 2. 3. Medium transparent materials – (Dentins – Groups A, B, C, D) These are universal composites of medium transparency. Dentins usually occupy about 85–90% of the volume of the entire restoration and are the basis for all types of restorations. The materials are color coded according to the VITA scale and are presented in various shades. Group A. Statistically, the colors in this group are used most often. Therefore, it can be defined as the main one. According to various studies, shades of group A occupy 80–85% of the color space of natural teeth, therefore the NanoPaq material presents the necessary colors in full: A 1, A 2, A 3, A 3.5, A 4 (Fig. 6). A special feature of this group of materials is the presence of special cervical shades of the composite. They are coded NA (N – neck – neck of the tooth). You can use: NA 2/3 - an intense color between A 2 and A 3 and NA 4 - a more intense color than A 4. These materials have the same transparency as regular Dentin, but their color is much richer, which means they look darker. By combining with other shades, you can easily achieve a natural, deep color on the necks of your teeth. Group B. They are found quite often, so all shades are also offered in this group: B 1, B 2, B 3. The following groups of the VITA scale are relatively rare, therefore they are represented only by the most common colors in their group.
Group C (dim yellow-gray teeth) is represented by C 2 Group D (rich yellow-brown) offers D 3 4. Highly transparent materials - (Artificial Enamels - In.) Highly transparent shades of NanoPaq material are necessary to imitate the cutting edge and give the restoration the most natural appearance . Artificial enamels have varying degrees of light transmission. The line of artificial enamels is represented by the following set: 1. Material with the maximum degree of transparency (InTr - Incisal Transparent) - this material has the maximum degree of transparency potentially possible. It is practically devoid of an opalescent effect; on the contrary, it can give a gray tint due to transparency and the influence of the dark background of the oral cavity. It is used where it is necessary to create volume of the tooth without changing the color or in cases where the enamel has pronounced transparency. This material has proven itself to be excellent when applied to the slopes of mounds when filling class I and II cavities. 2. Opal material with medium transparency (InU - Incisal Universal) - this material has a fairly high transparency, but still has an opal effect. It is often used as a universal one. Can be used in all cases (front and lateral teeth) when it is necessary to imitate ordinary light, medium-transparent enamel. The two types of enamel listed are basic (Fig. 7). The following enamels can be classified as auxiliary.
3. Light material with low transparency (InW – Incisal White) – light enamel with a pronounced opal tint. Rarely used without combination with others. Does not have pronounced transparency. 4. Enamel for whitened teeth (InBl – Incisal Bleach) – White enamel. Used to restore whitened teeth or teeth with very light enamel. When modeling, for the best effect, it is advisable to combine it with InTr. 5. Enamel with a yellowish tint
(InY – Incisal Yellow) – Well imitates the enamel of elderly patients, does not have high transparency, it is also advisable to combine it with InTr. 6. Warm pink enamel (InR - Incisal Red) - Is a translucent material that can be used for the restoration of teeth that have cold, dark shades. The application of such enamel makes the tooth more natural, with a “warmer” color. Highly transparent materials imitate natural enamel well, but the best result can only be achieved by combining them.. The artificial enamel options of this composite are sufficient for the most demanding dentist (Fig. 8). To make it easier to select the desired color, SCHUTZ Dental Group offers special shades made from the same NanoPaq composite material. The color patterns are wedge shaped. This is done so that transparency can be controlled depending on the thickness of the selected layer (Fig. 9).
In addition to knowledge about the aesthetic features of the material, it is necessary to evaluate its physical and mechanical properties to make an informed choice. This is the second criterion for choosing a filling material. These properties depend on the internal structure and composition of the material and characterize its hardness, toughness, flexibility, strength, etc. They are set by the manufacturer during production and cannot be significantly changed by the doctor. The predominance of the proportion of the polymer matrix in the composite makes the material highly plastic when modeling, but increases the overall polymerization shrinkage, negatively affects the resistance to mechanical loads, and also reduces the color stability of the final restoration. The more the material is filled with inorganic particles, the less its shrinkage will be, and the material itself will be stronger. But the maximum filling of the matrix with microparticles makes the material “dry” and has little plasticity. It becomes more difficult to work with (remember all the “packing” composites). A solution to this problem was found with the introduction of the latest developments in the field of Nanotechnology into dentistry.
NanoPaq is just such a composite. In addition to traditional micro-particles, its polymer matrix contains inorganic ceramic components with a diameter of 5 to 20 millionths of a millimeter (1 nanometer - 1x10-9 m) (Fig. 10).
This increases the filling density of the matrix without significantly changing the ductility of the material. The proportion of inorganic particles in such a composite increased to 83%, while the resin content decreased. This significantly reduced the volumetric shrinkage of the material and increased its strength. Thanks to the nano-structure, the surface area of the silanized particles increased by 10,000 times. This material holds its shape well during modeling and does not “flow around” in the oral cavity. In addition, the ceramic nanoparticles of this material are bound into agglomerates and the load is distributed over a larger area, which increases the overall service life of the restoration. Having a dense homogeneous structure, NanoPaq is highly polished, especially if you use the NanoPaq Polish polishing paste system. The abrasive size of these pastes is selected in such a way as to achieve a good dry shine in the shortest possible time (Fig. 11).
The structure of the nano-material allows it to maintain such shine for a long time. Choosing the material that is right for you is not an easy task. Some doctors are constantly searching and change composites every six months. This tactic is unjustified, since you need to get used to the material and feel it. And only by acquiring personal clinical experience and analyzing long-term results can one objectively evaluate the selected composite material. We have made our choice! We wish the same for you!
Article provided
Alternative methods for restoring anterior teeth
If for some reason it is not possible to restore a damaged tooth using filling material, you can choose another more acceptable option.
Veneers, lumineers
Overlays are made of ceramic or composite reflective materials
Veneers or lumineers are an alternative method of restoration of the frontal zone.
The material is recommended for installation in cases of uneven enamel color, existing displacements, increased abrasion, enlarged cracks and chips.
The overlays are made of ceramics or composite reflective materials.
The process of installing veneers involves grinding down the tooth enamel so that the thickness of the tooth after restoration is not too large. The impression made after turning helps to accurately replicate the existing reliefs on the working surface.
This promotes a tight fit of the insert, which increases the service life. The entire restoration procedure takes a little longer than using filling material.
This is due to the need to make an onlay based on an individual impression. It’s quite possible to fit it into 2-3 visits to the doctor.
The service life of veneers is on average 7-10 years, ultra-thin lumineers will last even longer - up to 20 years.
Crowns
To install crowns, grind adjacent teeth in a row.
In particularly difficult cases, specialists resort to traditional restoration methods, for example, installing a crown.
This option is indicated for severe tooth displacement or severe destruction.
The following materials are used in the process:
- porcelain;
- metal ceramics;
- zirconium dioxide;
- aluminium oxide.
To install crowns, grind adjacent teeth in a row. The question also arises about the removal of dental nerves, which can cause inflammation (pulpitis) after the crown has been fixed.
In case of severe tooth decay, it is restored using filling material. If it is completely absent, then an implant is first implanted into the bone tissue.
The process of making a crown according to individual parameters takes some time, so the patient is offered the installation of a plastic crown.
The duration of the restoration procedure is several weeks (3-5 visits to the doctor). Depending on the material used, the period of wearing the insert is determined; crowns made of zirconium dioxide will last longer than others (more than 20 years).
When deciding on the type of material and restoration method, it is worth considering that the invested funds are justified by aesthetic indicators and long-term operation. Therefore, savings in this matter should be reasonable and justified.
Tabs
An inlay is one of the most familiar types of filling. This method is most often used to restore the internal part - the chewing part, therefore it is used on molars. Inlays can be temporary, made of more fragile materials, or permanent, made of metal or ceramics. In some cases, the inlay not only fills the missing part, but also covers entire parts of it, but no more than half the surface of the tooth.
Pins
Pins are used in cases of severe destruction. Even if a stump has formed on the gum instead of a tooth, this method will help restore it. This applies to both front and side teeth. The pin itself resembles a metal needle or knitting needle that is inserted into the root canal. A metal rod writhing above the gum will become the basis for the restored tooth. The anterior ones use one pin, and the chewing ones use two.
Differences between the restoration of anterior and chewing teeth
When working with the frontal area of the dentition, aesthetics is primarily important; the use of composite veneers is relevant for them. Chewing teeth require maximum strength. Their restoration can be carried out with support from intra-root pins so that the structure is as strong as possible. For moderate damage to the crown, inlays are used, while for severely damaged teeth it is best to use crowns. Dentures reliably protect teeth, preventing their further destruction.
How much does it cost to restore a tooth?
As for how much restoration costs in Moscow, it all depends on many factors: the degree of destruction of hard tissues, the chosen technique, materials, the need to install a pin, stump or implant, as well as the level of prestige of the dental clinic. The difference in prices is significant, so each situation must be considered individually.
Restoration of an almost completely destroyed crown
If we talk about complete restoration using the direct method, then in this case the final cost will include several components at once. The procedure will require the following expenses:
- anesthesia - about 350 rubles,
- insulating gasket (cofferdam) - approximately 600 rubles,
- consumables (sterile kit) – 150 rub.,
- fixing a fiberglass pin (WDW) – RUB 1,500,
- restoration with composite materials – 3500-5000 rubles.
The photo shows the restoration of an anterior tooth using a fiberglass pin.
And this does not include preliminary preparation, which necessarily involves professional cleaning of plaque and deposits. You can save money on certain items. So, for example, in some cases, a fiberglass pin can be replaced with a regular anchor (metal), but then the restored area will no longer look natural and natural. This is not important for the chewing area, but it can affect the appearance of the smile. If you focus on aesthetics and then give preference to fiberglass, then the total cost of treatment will be about 6-8 thousand rubles.
Restoring half of a damaged crown
If only half of the tooth needs to be restored and there is no need to install a pin or core tab, it is enough to simply subtract the cost of these components. Classic direct extensions in this case will cost approximately 4000-4500 rubles.
Filling and restoration of a chipped incisal edge
When it comes to restoring defects resulting from caries, filling is most often used. Fixing one light filling will cost the patient approximately 2-3 thousand rubles, depending on the size of the cavity. But installing a ceramic or zirconium inlay from Onlay/Inlay will cost approximately 15 thousand rubles. The difference in price is significant, but here it must be taken into account that the latter method is used in cases of extensive destruction and for maximum tooth preservation. As for correcting the incisal edge with light polymer, the cost of this procedure usually varies between 1500-2000 rubles.
and the photo shows the installation of a light seal
Hiding defects with veneers and lumineers
Installation of one veneer made of E.Max ceramics costs about 30 thousand rubles. A product on a zirconium dioxide frame will cost 40 thousand rubles for fixation on one tooth. One lumineer made from Cerinate material costs about 65 thousand rubles, and a template DUO will be slightly cheaper - 40 thousand rubles for one overlay. A budget option that will give no less high-quality and aesthetic results is a ceramic composite - you will have to pay 25 thousand rubles for installing one overlay made of this material.
Prosthetics with crowns – turnkey prices
Correction of the smile area is always more demanding, since in this case it is important to ensure the proper level of aesthetics - the result must be as natural as possible and at the same time long-lasting. Therefore, more expensive materials are used
The table below shows approximate prices for aesthetic single prosthetics.
| Material | Approximate price, rub. |
| Metal composite | from 5 to 15 thousand |
| Metal ceramics | from 5 to 15 thousand |
| Ceramic composite | 20 thousand |
| E-max | 30 thousand |
| Zirconium | 30 thousand |
Prices are indicated in a turnkey format - this usually includes an initial consultation, taking impressions, anesthesia, consumables, creation of an orthopedic structure and its installation. You may have to pay separately for x-rays and pain relief - it is better to clarify all the details directly at the clinic. In some dental centers, the cost of a temporary crown is not included in the total amount, which is approximately 1000-1500 rubles. As for the cost of prosthetics on implants, this is described in detail in our separate article.
Dental community
21.06.2020, Site section: Current articles. Dentistry. Health care organization. Right.
“Pediatric Dentistry and Prevention”, No. 2 - 2020
Skripkina G.I., Doctor of Medical Sciences, Associate Professor, Head of Department Garifullina A.Zh., Candidate of Medical Sciences, Associate Professor Breslavskaya E.A., Clinical Resident
Department of Pediatric Dentistry, Omsk State Medical University
Summary
Relevance: Light-curing composite materials have a large number of indications for use and are actively used by dentists in clinical practice. The properties of these materials vary depending on their composition and filler size. We conducted a survey of dentists and therapists in public and private dental clinics in Omsk to determine the compliance, objective indicators of the physical and chemical parameters of the composite materials under study and their subjective assessment by doctors using these materials in their work.
Purpose: comparison of objective indicators of various properties of photocomposite materials with the subjective assessment of dentists.
Material and methods: study of the physicochemical properties of light-curing composite materials most often used in the practice of Omsk dentists in public and private clinics. A research design was developed and a survey of 148 dentists in Omsk was conducted to determine the subjective assessment of these materials.
Results: a comparative analysis of objective and subjective indicators of composite materials was carried out.
Conclusions: the data on the physical and chemical parameters of photocomposite materials fully correspond to the subjective assessment of dentists in Omsk.
Key words: Dental materials, composite materials, fluid-flowing composites, properties of materials, survey, questionnaire, dentists.
Introduction
Modern practical dentistry predominantly uses dental photocomposite filling materials for the treatment of carious and non-carious dental lesions due to their positive aesthetic and mechanical characteristics [1, 2, 3, 4]. Composite materials allow the doctor to carry out gentle preparation of teeth, restoration of teeth with defects of various shapes and configurations and have a number of physical and chemical advantages: high aesthetic properties, high strength, a wide range of colors [5, 6, 7], the ability to model and give an anatomical shape to the damaged crown part of the tooth, a stronger connection with the hard tissues of the tooth, better marginal adherence to the hard tissues of the tooth, biological tolerance to the tissues of the oral cavity [8, 9, 10, 11, 12, 13]. But such materials are also imperfect and are constantly being improved [14, 15, 16, 17].
The purpose of the work is to compare data on the objective physical and chemical properties of a number of composite materials with a subjective assessment of the same materials, in order to formulate practical recommendations for dental therapists.
Objectives: 1. Assessment of physical and chemical parameters of a number of composite materials. 2. Determination of subjective assessments of photocomposites by dentists in Omsk. 3. Analysis of objective and subjective parameters to formulate practical recommendations for dentists and therapists.
Material and research methods
Today, the market offers a huge selection of photocomposite materials from various manufacturers, both foreign and domestic. For the study, materials were selected that are most often used in the practice of Omsk dentists in public and private clinics based on the data obtained from a questionnaire survey in order to give a personal subjective assessment of these products.
The following methods were used in the work: sociological, analytical. We developed a research design and developed a questionnaire to compare the subjective assessment of composite materials with their physicochemical parameters.
Studies of the objective physical and chemical properties of the materials under study were carried out in June 2021 by a certified tester under the supervision of the head of the Research Center B.V. Ryabokon. The tests were carried out in accordance with national standards: GOST R 56924 - 2021 (ISO 4049 - 2009) “Dentistry. Polymer restorative materials" and GOST 31574-2012 "Dental polymer restorative materials". An objective assessment of the properties of materials is represented by the following parameters: depth of curing, diametric tensile strength, bending strength, consistency.
Our work involved the evaluation of the following composite materials (names/characteristics correspond to official registration documents):
- Filtek Ultimate Universal (3M ESPE) is a universal restoration material.
- Estelux NK (Stomadent) is a nanohybrid composite material.
- DentLight (VladMiVa) – microhybrid composite.
- Filtek Ultimate Flowable (3M ESPE) is a fluid-flowing restoration material.
- FlowRest (Stomadent) – low-modulus (flowable) composite
- DentLight Flow (VladMiVa) is a flowable composite.
Materials differ not only in price category, but also in their properties, which are reflected in the work process and its results. For the first three positions (packable composites) in the official registration documents, only the Estelux NK material from the Stomadent company contains the word “nanohybrid”; but in two other cases, both manufacturers position these products as “nanocomposites” and as materials made with the use of nanoadditives, as indicated on the manufacturers’ websites, as well as in their catalogs and presentation materials.
Research results and discussion
A questionnaire survey was conducted among 148 dental therapists in Omsk. In government institutions, the number of respondents was 92. Of these, 44.44% had work experience of more than 10 years, 22.22% had 5-10 years of experience, and 33.33% had less than 5 years of experience.
The number of surveyed doctors from private clinics is 56. The smallest number of them - 9.52% - are specialists with more than 10 years of work experience, 38.09% have less than 5 years of experience and the majority - 52.38% - have been working for 5-10 years.
When carrying out restoration, 59.25% of dental therapists in public clinics use a combination of condensed and liquid (flowing) composites, the remaining 40.74% use only condensed composites. In private institutions the situation is very different. The combination of “condensable and liquid (flowable) composites” is used in restoration by 95.23% of doctors.
The largest number of surveyed doctors from public and private clinics - 85% - use fluid-flowing composites when sealing fissures. 78% use these materials when filling using the layer restoration method. 77% - to restore minor enamel chips. 59% of doctors prefer liquid materials when filling Black class 2 cavities using the tunnel preparation technique. There was a slight majority of votes in favor of private practice. When restoring the marginal seal of fillings, flowable composites are used by 50% of doctors. Small cavities on the chewing surface are filled with liquid materials by 59% of surveyed doctors. Wedge-shaped defects and damage in the cervical part – 43%. Black class cavities 3 and 4 – 30%. 36% of respondents fix fiber systems and 21% fix splints using flowable composites. Most of them are doctors at private clinics.
Doctors use condensed composites in the following clinical situations. 95% use these materials to fill cavities of class 1 and 2 according to Black. 78% - when filling using the layer restoration method. 91% of doctors model the tooth stump with condensed composites. The smallest number of doctors in both groups – 13% – use these materials in the manufacture of indirect restorations. In the last two cases, there is a slight advantage in favor of private clinics.
An objective assessment of the properties of materials is reflected in Table No. 1 and is represented by the following parameters: depth of curing, diametric tensile strength, bending strength, consistency. In the note column, a description of tactile properties and strength is highlighted.
Table 1. Objective assessment of the physicochemical properties of the materials under study
| Name of material, Color of material | Curing depth, h mm | Strength at diametrical rupture, MPa (not less than 34 MPa) | Bending strength, MPa (not less than 80 MPa) | Consistency, mm | Note | ||||
| According to the manufacturer's instructions | h, mm in 10 sec. | ||||||||
| Curing time sec. | h, mm not less | h, mm actually | |||||||
| 1. | Filtek Ultimate Universal Restorative, EA3 | 20 | 2 | 2, 57 | 2, 18 | 60, 9±4, 3 | 119, 7±19, 3 | 16.5x16.5 | + Dense, but very flexible, easy to model, high strength. — Chips on the cured sample. |
| 2. | DentLight, DA3 | 30 | 2 | 2, 03 | 1, 60 | 48, 5±6, 5 | 108, 5±21, 0 | 19, 0х20, 0 18, 5х19, 0 | — Less ductile, long curing time, wide range of values (flexural strength) |
| 3. | Estelux NK, EA3 | 20 | 2 | 2, 76 | 2, 28 | 54, 0±3, 1 | 108, 4±8, 8 | 19.5x19.5 | + Plastic, easy to model |
| 4. | Filtek Ultimate Flowable Restorative, A3 | 20 | 2 | 2, 16 | 1, 85 | 52, 5±5, 0 | 117, 1±7, 3 | 30, 0x30, 0 | + Thixotropic, non-spreading, high strength |
| 5. | DentLight-Flow, A3 | 30 | 1, 5 | 2, 87 | 2, 15 | 38, 2±8, 0 | 83, 8±2, 9 | 40.0x40.5 | — Highly flowable, not thixotropic, long curing time, near minimum strength |
| 6. | FlowRest, A3 | 20 | 2, 0 | 2, 27 | 1, 86 | 42, 4±3, 2 | 95, 7±4, 5 | 26.5x26.5 | + Thixotropic, does not bleed |
Tests were carried out in accordance with the requirements of national standards:
- GOST R 56924-2016 (ISO 4049-2009) “Dentistry. Restorative polymer materials";
- GOST 31574-2012 “Dental Polymer restorative materials. Technical requirements. Test methods clauses 6, 12.
The material Filtek Ultimate Universal (3M ESPE) and DentLight Flow (VladMiVa) were used equally by doctors of private and public institutions, Estelux NK (Stomadent), DentLight (VladMiVa) and FlowRest (Stomadent) were used by the majority of doctors in public clinics, Filtek Ultimate Flowable (3M ESPE) – most doctors in private clinics.
According to objective indicators, among the packaging materials studied, Filtek Ultimate Universal and Estelux NK are practically at the same level. Filtek Ultimate Universal has better diametric tensile strength and flexural strength, but greater actual cure depth and 10 second cure depth. has Estelux NK. These indicators are directly reflected in the wear resistance and satisfaction with the quality of the restoration and its long-term results - both materials received the highest rating. In Table 1, in the notes column, among the advantages of the Filtek Ultimate Universal material, its density is indicated and fully corresponds to the doctors’ assessment of “excellent” for this property. The Estelux NK material received the same rating. Excellent ductility and modeling of these materials are listed as pluses among objective indicators and correlate with the doctors’ answers. Based on the “Adhesion to the instrument” parameter, doctors concluded that Filtek Ultimate Universal adheres to the instrument less than Estelux NK and DentLight. Filtek Ultimate Universal and Estelux NK are better polished than DentLite (see diagram 1). The Dentlight material, according to objective data, has a longer curing time, a smaller curing depth and diametric tensile strength than other tested representatives of packable composites. The disadvantages of this material include a wide range of bending strength values. For most of the properties assessed by doctors, this material was rated “good”, which is a consistently good result.
Diagram 1. Results of subjective assessment of the properties of packaged composite materials using a 10-point system
Among the studied fluid composites, according to the objective data in Table 1, the last position is occupied by the DentLight Flow material. FlowRest is objectively inferior to Filtek Ultimate Flowable material in terms of bending strength and diametrical tensile strength. The latter has an average consistency index among the fluid materials under study. According to survey responses from dentists, FlowRest received the largest number of “excellent” and “good” ratings. This material is thixotropic and does not spread (see Table 1); therefore, it is convenient for insertion and removal from the cavity. It should be noted that only 8% of the total number of doctors used this material. Filtek Ultimate Flowable is also thixotropic and does not spread, which doctors noted, rating the parameters “Plasticity” and “Ease of insertion and removal from the cavity” as “good”. In general, the doctors surveyed who used this material were satisfied with the quality of the restorations. DentLight Flow received the majority of “satisfactory” ratings from doctors; not a single property was identified that was completely dissatisfying to the respondents. All flowable materials were rated “satisfactory” according to the modeling parameter, which is logically explained by their physicochemical properties (consistency, fluidity) and indications for use (see diagram 2).
Diagram 2. Results of subjective assessment of the properties of fluid composite materials using a 10-point system
conclusions
Based on the data of a subjective assessment of the studied materials, obtained during a questionnaire survey of dentists and general practitioners in the city of Omsk, and taking into account the objective assessment of their physical and chemical parameters, we made the following conclusions. These physical and chemical parameters are fully consistent with the subjective assessment of dentists. Among the group of packable composite materials, according to objective criteria, the leading position is occupied by Filtek Ultimate Universal (3M ESPE), this is confirmed by the answers of dentists. Estelux NK (Stomadent) takes second place in terms of objective parameters, but, according to the subjective assessment of doctors, it is practically not inferior to the leader.
When evaluating liquid-flowing materials, doctors gave preference to FlowRest (Stomadent). It is necessary to take into account the fact that this is only 8% of respondents. Filtek Ultimate Flowable (3M ESPE) is ahead of FlowRest by objective assessment, but takes second place by subjective assessment. Doctors are equally satisfied with the quality of restorations using both materials.
We recommend packable materials for clinical use - Estelux NK, Filtek Ultimate Universal and flowable materials - FlowRest and Filtek Ultimate Flowable for private and public dental institutions, taking into account the peculiarities of the pricing policy.
Bibliography
- Aleynikov K.V., Vagner V.D. Efficiency of dosing light-cured composite materials using standard and modified methods // Dentistry for everyone. 2010, 4, 16-18.
- Vikulin A.V., Markin A.V. Results of using low-modulus light-cured composite material “Flourest” to restore the gingival margin // Dental Forum. 2012, 5, 35.
- Vasilenko A.V., Vikulin A.V., Ibragimov T.I., Stetsyura O.A. Application of light-curing hybrid composite material for aesthetic restoration of the gingival margin // Dental Forum. 2016; 4, 18.
- Getsman A.V. Restoration of temporary incisors of the upper jaw // Pediatric dentistry and prevention. 2015; 14; 4 (55), 17-18.
- Blokhina A. A. Options for solving the current problem of restoring cavities in lateral teeth // DentArt. – 2012; 1, 52-57.
- Danilova M.A., Machulina N.A., Shevtsova Yu.V., Kamenskikh D.V. Clinical and experimental rationale for the use of various filling materials in preschool children // Pediatric dentistry and prevention. 2019; 19; 2(70), 31-36.
- Maslak E. E. Prevalence of dental caries and modern directions of caries prevention // Medical alphabet. 2015; 1; 1, 28-31.
- Nikolaenko S.A., Pechenegina E.V., Zubarev A.P., Fedorov Yu.V., Lobauer U. Comparative characteristics of the wear resistance of modern polymer composites // Clinical dentistry. 2021, 3 (83), 4-9.
- Mochalov Yu. A. Methodological approaches to the clinical assessment of dental photocomposite filling materials as medical products // Universum. Medicine and dentistry. 2021, 9(64).
- Caixeta RV, Guiraldo RD, Kaneshima EN, Barbosa AS, Picolotto CP, Lima AE, Gonini Junior A, Berger SB. Push-Out Bond Strength of Restorations with Bulk-Fill, Flow, and Conventional Resin Composites. 2015;2015:452976. doi:10:1155/2015/452976.
- Furuse A., Gordon K., Rodrigues F. et al. Watts Color-stability and gloss-retention of silorane and dimethacrylate composites with accelerated aging. — J. Dentistry, 2008, v. 36, No. 11, r. 945-952
- Monterubbianesi R, Orsini G, Tosi G, Conti C, Librando V, Procaccini M, Putignano A. Spectroscopic and Mechanical Properties of a New Generation of Bulk Fill Composites. Front Physiol. 2016 Dec 27; 7, 652. doi: 10:3389/fphys.2016, 00652.
- Radhika M, Sajjan GS, Kumaraswamy BN, Mittal N. Effect of different placement techniques on marginal microleakage of deep class-II cavities restored with two composite resin formulations. J Conserv Dent. 2010; 13, 9-15.
- Skripkina G.I., Garifullina A.Zh. Clinical examination as the main clinical approach to the prevention of dental caries in children // Dentistry. 2015;94;5:64-66.
- Skripkina G.I., Garifullina A.Zh., Mityaeva T.S., Romanova Yu.G., Mikhailovsky S.G., Dmitrieva V.A. Experience in the use of dual-curing composite material for fixation of fiberglass pins and restoration of the tooth stump in the practice of a pediatric dentist // Endodontics Today. 2015; 3, 35-37.
- Korolenkova M.V., Arzumanyan A.P. Comparative analysis of microleakage of fillings and standard pediatric crowns during the restoration of temporary molars after simulated pulpotomy // Pediatric Dentistry and Prevention. 2019;19;1(69):46-50.
- Effect of surface sealants on marginal microleakage in Class V resin composite restorations / SV Silva Santana // J. Esthet. Dent. - 2009. - Vol. 21, No. 6. - P. 397-404.
Conflict of interest: The authors declare no conflict of interest
Received: February 11, 2021
Skripkina Galina Ivanovna – Doctor of Medical Sciences, Associate Professor, Head of the Department of Pediatric Dentistry of the Federal State Budgetary Educational Institution of Higher Education "Omsk State Medical University" of the Ministry of Health of the Russian Federation For correspondence
Garifullina Albina Zhamilievna – Candidate of Medical Sciences, Associate Professor, Associate Professor of the Department of Pediatric Dentistry of the Federal State Budgetary Educational Institution of Higher Education "Omsk State Medical University" of the Ministry of Health of the Russian Federation For correspondence
Breslavskaya Evgeniya Aleksandrovna – clinical resident of the second year of study of the Department of Pediatric Dentistry of the Federal State Budgetary Educational Institution of Higher Education "Omsk State Medical University" of the Ministry of Health of the Russian Federation For correspondence
Views 696 Likes 0 Likes
What is dental restoration with filling material?
Artistic restoration of anterior teeth: composite aesthetic restoration and the use of veneers
The concept of “restoration” itself, translated from Latin, has two definitions, which are united by one word - restoration.
In dentistry, the term means giving a tooth an anatomical shape and color while maintaining functional loads.
Artistic restoration with filling material is a procedure that is performed at the final stage of treatment.
It involves filling the tooth cavity with a special solution to install a filling.
This type of work is used for various lesions, in particular caries. The filling material replaces the missing fragment of the tooth, preserving its functions.
The greatest professionalism and skill is required when performing restoration using filling in the front, because one of the tasks is to give the jaw an aesthetic appearance.
Restoring the integrity of the frontal group of teeth using filling material is done in the following cases:
- destruction of enamel and tissues;
- presence of chips;
- if the color has changed;
- hypoplasia (underdevelopment of tissues);
- if there is a need for aesthetic alignment of the tooth surface (congenital or acquired defect);
- if there is a gap between the teeth;
- for restoration of enamel after removal of affected fragments, including after treatment of caries.
The difference between filling and tooth restoration
Restoration of the anterior and chewing teeth with filling material allows you to restore the anatomical shape, integrity and functionality of the dental crown. In fact, a filling performs approximately the same functions. But there are still differences between these two recovery methods, and they are significant:
- Filling involves, first of all, restoring the functional parameters of dental tissues, and tooth restoration is aimed at restoring not only functionality, but also aesthetics - materials are selected in such a way as to most accurately imitate natural dentin and enamel, their color and degree of transparency.
- Installing a filling is a purely therapeutic procedure, while restoration procedures combine both treatment and artistic restoration.
- Fillings are installed when no more than a third of the crown of the tooth is destroyed. Restorative measures can be carried out in cases of more significant destruction of the crown, as well as in cases where the dental crown is visually intact, but it is necessary to correct its shape, color, or correct wide interdental spaces.
Postoperative sensitivity
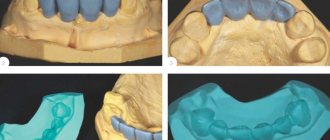
A peculiarity of working with vital teeth (Fig. 11-16) is the occurrence of postoperative sensitivity after fixation of permanent crowns or covering ceramic inlays. In this case, one of the possible causative factors may be cement for fixing fixed prostheses [46]. Errors when performing adhesive preparation of hard tissues of vital teeth before using composite cements can lead to postoperative sensitivity and even pulp death [3,40]. It has been established that the use of self-adhesive cements is characterized by a low incidence of postoperative sensitivity [14,44].
| Rice. 11. Initial clinical situation: secondary caries and hard tissue defects were found on vital teeth after removal of old stamped crowns | Rice. 12. After treatment of caries, the core part of the teeth was restored with double-curing core material LuxaCore Dual (DMG, Germany), while the vitality of the teeth was preserved | Rice. 13. View of the teeth before taking an impression, retraction thread is placed around the teeth |
| Rice. 14. Fragment of a two-stage two-layer impression with a detailed display of the boundaries of the preparation and the periodontal sulcus | Rice. 15. Metal-ceramic and solid-cast crowns on the model | Rice. 16. Crowns after fixation with permanent cement. SCC was chosen to prevent the occurrence of postoperative sensitivity |
D. Saad et al. (2010) found a lower incidence of postoperative sensitivity with self-adhesive cements compared to classical composite cements that require etching and preliminary adhesive preparation. Of interest is a study conducted by CA de Souza Costa et al. (2008), who compared the effect on the dental pulp of two SCC cements and a composite one with the etching stage and adhesive preparation. On 32 premolars to be removed for orthodontic reasons, cavities were formed and ceramic inlays were fixed using the above cements, after which these teeth were removed (after 7 and 60 days) and a histological examination of the dental pulp was performed. It was found that the use of traditional composite cement with the stage of etching and adhesive preparation is accompanied by a more pronounced effect on dental pulp tissue compared to SCC.
N. Denner et al. (2007) conducted a comparative study of the incidence of postoperative sensitivity in vital teeth after fixation of full crowns using 2 types of cements: glass ionomer (GIC) and SCC. 120 crowns were installed in 30 patients, and a comparative analysis of such an indicator as postoperative sensitivity after 24 months did not reveal a difference in the use of both cements. M. Blatz et al. (2013) studied the incidence of postoperative sensitivity in vital teeth after fixation of full crowns using SCC and polymer-modified GIC. The incidence of postoperative sensitivity was lower when fixing crowns with SCC compared to GRC modified with polymers.
Approximate prices
How much restoration will cost directly depends on the scale of the problem and the chosen restoration method. If the damage is minor, such as a small chip on a front tooth, then the cost of restoring its shape using the direct method will be about 1,500-2,000 rubles. This includes anesthesia (250-350 rubles) and light-polymer material (about 1000 rubles). It’s another matter if the crown is destroyed by more than half. The cost of such a restoration without installing a pin will be approximately 3500-4000 rubles. Restoring a completely destroyed crown consists of the following components:
- use of anesthetic – 250-350 rubles,
- rubber dam (isolation of the working area from saliva) – about 600 rubles,
- sterile kit for a doctor – 150 rubles,
- recreating the anatomical shape of a tooth using light-curing composites – 3500-5000 rubles,
- installation of a fiberglass pin – 1500 rubles.
The total cost of complete tooth restoration in Moscow varies from 5 to 7 thousand rubles. Pricing is also influenced by the individual characteristics of the clinical picture, the status of the dental clinic, and the region of treatment.
Separately, you can consider the current prices for veneers made from different materials. Approximate prices are presented in the table below.
| Types of modern veneers | Approximate prices for 1 veneer |
| E.max ceramic | 30 thousand rubles. |
| Zirconium veneers | 25 thousand rubles. |
| Ceramic composite linings | 20 thousand rubles. |
| DUO | 45 thousand rubles. |
| Cerinate | 65 thousand rubles. |
There is also an option with lumineers - they are even thinner than veneers, but do not require grinding of living enamel and allow you to create the smile of your dreams in just a couple of visits to the dentist. True, such a restoration will cost an order of magnitude more.
Today there are many opportunities to create a truly Hollywood smile - snow-white and flawlessly even. Another thing is that such radical measures require quite impressive financial investments. If artistic restoration is not a whim for you, but a necessity, then carefully choose a clinic and a doctor to get a high-quality, aesthetic and durable result.
Methods of composite dental restoration
The choice of restoration method with light-curing substances depends primarily on the type of tooth affected (anterior/frontal or chewing) and the extent of damage.
Veneers
Veneers are thin plates of composite or ceramic that cover the dental surface. This is done either to correct visual dental defects or to protect against external damage. The aesthetic function of veneers is to mask widened tooth gaps or pronounced yellowness of the enamel. They are made by a dental technician or, in some cases, formed by a dentist directly in the patient’s oral cavity using a direct method.
After local anesthesia, the dentist removes part of the enamel so that the veneer does not extend beyond the dentition. Then the contact surface is cleaned, degreased, and treated with an antiseptic. The composite is applied in layers, drying each with a special directional lamp. The final stage is to grind its surface, give it a physiological shape corresponding to the configuration of the tooth, and cover the surface with fluorine-containing varnish.
Tabs
The inlay is represented by a composite cast, duplicating the shape of the tooth, made by the indirect method. Inlays are necessary to close the dental cavity.
Installation of a composite inlay is carried out in two stages. On the first visit, the doctor treats the affected tooth. There is no need to grind down healthy tooth areas. Then an impression of the dentition is taken to establish the outlines of the tooth and bite, the color of the future inlay is determined and its temporary analogue is installed. An inlay is then made from a composite material based on the shape of the impression, which is installed during a follow-up visit to the dentist. Installation is carried out using special adhesives. The border of the inlay is carefully polished so that it blends with your own tooth.
Currently, this technique is rarely chosen due to its low efficiency compared to inlays made from other materials. However, the cost of the procedure remains quite high.
Seals
Before installing a composite filling, the dental cavity is first prepared: the damaged tooth area is drilled out and the cavity is given the proper shape, and the surface is cleaned for a tighter bonding of the composite. The tooth is isolated, limiting contact with liquid media, and etched for 15 seconds using phosphoric acid, after which the enamel should become dull.
Then a binding component is applied, hardening under the influence of a photopolymerizer, and the composite substance is directly installed. The elastic or flowable composite is applied in layers, the layer thickness should be about 2 mm so that it hardens properly under the influence of the light lamp. When applying layers, the dentist gives the composite the physiological shape characteristic of the tooth in order to preserve the aesthetic appearance. Before the final polishing, the bite is checked so that the protruding elements of the filling do not interfere with chewing; they are ground off. Polishing gives the material smoothness and shine.
Table. The choice of restoration method depending on the shape and stage of tooth decay
| Degree of destruction | Central (or internal) caries | Peripheral (or external) caries | Combined central + peripheral |
| Minimum | Amalgam or composite material, pin | Amalgam, composite material or polymer-modified glass ionomer | Amalgam, composite material or polymer-modified glass ionomer |
| Moderate | Amalgam on cement base | Amalgam, composite material or polymer-modified glass ionomer | On a large tooth there is an amalgam, on a small tooth there is a cast gold inlay |
| Heavy | Crown+contact rod | Crown | Crown+contact rod |
| Complete loss of a dental crown | – | – | Molars: crown + contact rod; premolars: root treatment+contact rod+crown |